Myocarditis and COVID-19 mRNA vaccines
The gist: Presently and primarily in younger males with the second dose, there appears to be a small increase in the risk of myocarditis with mRNA vaccination. This is definitely not a trivial matter and it needs to be taken seriously, but the concerns need to be weighed against the risks of COVID-19. To start with, COVID-19 is itself a known cause of myocarditis, and even if we take 12-17 year-old-males and the second dose of mRNA vaccine as a point of reference (available data suggest this is the group at greatest risk), the risk of myocarditis from COVID-19 (specifically from MIS-C, even factoring in its rarity) is significantly greater. Myocarditis has a very broad range of severity, ranging from asymptomatic to causing heart failure requiring a heart transplant in the most severe cases, or lethal heart arrhythmias and sudden cardiac death. However, thankfully, most cases of myocarditis do not reach that degree of severity, and fortunately the cases associated with the mRNA vaccine appear to be mild and transient: the vast majority of patients appear to have had temporary hospital stays (mainly for monitoring purposes) and were safely discharged with normalizations in their health. The severity of myocarditis depends a lot on the underlying immunological processes driving it and the preliminary data we have suggests that the form of myocarditis caused by the mRNA vaccines involves a type of immune cell that is generally regarded as being protective and associated with better outcomes in myocarditis, hinting that we may not see this evolve into more serious chronic health issues in most cases (but time will tell and continued follow up is needed). Dr. Rochelle Walensky, the current CDC director, recently clarified that if 1 million children are fully immunized with an mRNA vaccine, we may expect 30-40 cases of this transient, mild myocarditis. However, we will have prevented 8000 cases of COVID-19, 200 hospitalizations, 50 ICU stays and 1 death in this age group and thus the benefits far exceed the potential risks. Dr. Walensky is not just the CDC director but she is the mother of two teenage boys who have both been fully vaccinated. Because of these concerns, however, some have suggested that there should be modifications to how the vaccines are given to the at risk age groups. I have no problem with this in principle but these approaches absolutely must be driven by data. For example, some have argued that a single dose of vaccine may be adequate in these individuals, but there is no data to support that choice and it necessarily does carry the very probable risk of subpar protection in the face of increasingly communicable variants. Alternatively, others have suggested to extend the interval between the doses of vaccine- but here there is also no data. In terms of the immune protection generated by the vaccine, this is not an issue: longer intervals lead to superior antibody responses. However, we have no hard data that this results in a reduced risk of myocarditis and a longer interval means a longer period with incomplete protection, so such decisions should be made in the context of COVID-19 activity in the community, bearing in mind that it takes time for full immunity to be generated. There is also the possibility that the longer dosing interval may increase the risk of myocarditis because it causes a more robust immune response. For now, the best option is to vaccinate children as dictated by the schedules until data emerges to show otherwise. The myocarditis risk in question is clearly rare and there are a number of reporting biases that can be exaggerating its risk (see below for details), and while it isn’t nothing, the fact that the vast majority of cases have been mild and transient clearly indicates that leaving children unprotected or incompletely protected from COVID-19 is currently the bigger risk, especially in the face of the delta variant which seems to require two doses of vaccine for full protection and has substantially heightened transmissibility. If we elect to favor precautionary principles in our current precarious position, we very well may do far more harm than good.
On a personal note, I am a 23-year-old male with several risk factors for myocarditis generally in addition to my sex and age (though that alone puts me in the statistical bin at highest risk of myocarditis associated with the mRNA vaccines) who received 2 doses of the Pfizer/BioNTech vaccine exactly 3 weeks apart and had no side effects more serious than arm soreness and very restful sleep (not even fatigue- just slept more deeply at night) for about a day or two (in the case of the second dose) and I was aware of the signal in Israel at the time I was being vaccinated- but I know the risks to me from COVID-19 are so much higher. I don’t like to use anecdotes in matters of science, but this is a representative one. In the vast majority of vaccinations, after a few days (at most) of discomfort and side effects, patients are completely fine and have excellent protection against COVID-19.
Based on everything we know *right now* getting 2 doses of mRNA vaccine for your children as soon as possible is the safest thing for them. That may change as we learn more, but it’s important not to be rash and to lean on data in uncertainty.
This subject is complex because it has many moving parts. As I see it, to understand it one needs to understand myocarditis first, then COVID-19’s associated risk of myocarditis, and then what vaccine-associated cases of myocarditis look like to be able to accurately understand this matter. Of course, it’s also important to have a primer on how the heart works, so I have presented a brief summary of that first. For those who wish to skip the background (understandably as it is lengthy), “II: Myocarditis associated with COVID-19 Vaccines and the Risk-Benefit Analysis” is likely the best point to start reading.
0: Heart Physiology (very simplified summary)

Gourdie RG. The cardiac gap junction has discrete functions in electrotonic and ephaptic coupling: Gap junction function in cardiac conduction. Anat Rec (Hoboken) 2019;302(1):93–100.
Myocarditis is a disease of the heart, and so to understand it one first needs to have a basic idea of how the heart works. The heart is a muscular organ in the middle of the chest asymmetrically positioned towards the left side in most people, roughly the size of one’s fist, and is responsible for circulating blood throughout the body by acting as a pump. In doing this, it ensures that all the cells are nourished with oxygen and other key nutrients and also that metabolic waste products are removed and then cleared through other organs like the kidneys and the lungs. Contraction of the heart is controlled by electrical currents that are mediated by the flow of ions into and out of the heart’s cells (excitation-contraction coupling is the formal term). The heart muscle cells (cardiomyocytes) are linked to each other via gap junctions that allow the flow of ions between adjacent cells; this ensures that the current can travel seamlessly from one cell to the next adjacent cell so that a rhythmic contraction can result. The currents originate from a region of the heart called the sinoatrial node (SA node) via a pacemaker cell, and they then travel through to the atrioventricular node (AV node) where the current is paused to allow for proper contraction of the upper chambers of the heart (the atria) so that the lower chambers (ventricles, commonly abbreviated LV and RV for left and right ventricle respectively) may fill. The ion channels within the SA node are set up in such a way that they spontaneously generate a rise and fall in electricity without any cue required from the rest of the body, as long as the cells themselves are healthy. The current then travels down to the ventricles causing them to contract. The left ventricle ejects blood into the systemic circulation (throughout the body), whereas the right ventricle ejects blood into the pulmonary circulation (the lungs). Blood in the pulmonary circulation gets oxygenated and then returns to the heart at the left atrium, and then is transported through the body via the action of the left ventricle. Contraction of the heart is known as systole, and relaxation is known as diastole; proper timing of both phases is critical for proper heart function. The chambers of the heart fill during diastole, and the blood is ejected and circulated during systole. Arrhythmia refers to the state where the currents in the heart do not function in such a way that a healthy contraction occurs, but not all arrhythmias are equally serious and not all are treated the same. Defibrillation, for example, is an emergency treatment that is designed to rescue people from deadly heart rhythms, is only appropriate for pulseless ventricular tachycardia and ventricular fibrillation- it does not treat all arrhythmias.
To explain how well the heart is functioning quantitatively, we can use a few parameters. Stroke volume is the amount of blood that is ejected from the heart with each heartbeat, or stated more formally, it is the difference between the end-diastolic volume (the amount of blood in the heart at the end of diastole) and end-systolic volume (the amount of blood in the heart at the end of systole). Ejection fraction is the proportion of the blood that is ejected from the ventricles with each heartbeat, or more formally it is the ratio of the stroke volume to the end-diastolic volume (it is normally about 0.55 or 55%, but a healthy range is typically anywhere from 0.5 to 0.7); this metric is very important for gauging how effectively the heart pumps. Cardiac output is the product of stroke volume and heart rate: it is the amount of blood circulated by the heart in some specified time period. Two major forces affect the ability of the heart to pump blood: preload and afterload. Preload refers to the left ventricular (LV) end diastolic volume which reflects the tension applied to the left ventricular muscle cells before a contraction. Afterload refers to the pressure the ventricle must pump against in the aorta, the major blood vessel that supplies the body that branches directly off the heart. The Frank-Starling relationship essentially says that the volume of blood ejected from the heart by the ventricle depends on the volume present in the ventricle at the end of diastole, which depends on the volume of blood returned to the heart by the veins (venous return). Per the Frank-Starling relationship, all else equal, an increase in preload results in an increase in cardiac output, while an increase in afterload results in a decrease in cardiac output. This relates to the concept of contractility (more formally called inotropism) which is the ability of a cardiac muscle cell to build up tension at a given cell length. The more tension it builds up, the harder it can contract and therefore eject blood.
One major concern with myocarditis is that it can progress into heart failure, of which there are many kinds, and therefore what follows is not intended to be comprehensive (but you can see this for a more thorough discussion). Upon damage, the heart may not be able to pump as effectively which results in reduced cardiac output and a buildup of blood in the veins. Eventually, this leads to fluid retention, which depending on the extent is not always bad because it can increase preload which per the Frank-Starling relationship should increase cardiac output- thus even if the heart functions at half of its normal capacity, because of the increased fluid retention, as long as the patient is resting, cardiac output may in fact be normal. However, as heart failure progresses it can become a more significant problem because eventually the retention exceeds the compensation of the Frank-Starling mechanism, at which point blood flow to the kidneys is reduced, which impairs the ability to regulate electrolytes and regulate fluid volume. Heart failure is also a problem because it depletes cardiac reserve, which is the maximum percentage that cardiac output can increase above its normal state. In most people, cardiac reserve is about 300% (meaning that under vigorous exercise the cardiac output might quadruple, or increase by 3 times its normal amount; in athletes it can be about 500 to 600%), but in heart failure it can be depleted because the heart is working at its hardest at baseline. Ejection fraction can be helpful for assessing the severity of heart failure (but not in isolation). Heart failure would be expected to present with reduced ejection fraction (this type of heart failure is creatively termed heart failure with reduced ejection fraction or HFrEF). However, some forms of heart failure result in hypertrophy of the heart muscle (i.e. the muscle gets bigger) to compensate for the reduced cardiac output. This increases the ejection fraction but reduces the volume of the heart chambers, preventing adequate filling (preload) and thus heart failure occurs even though ejection fraction is preserved (this is creatively termed heart failure with preserved ejection fraction or HFpEF). In some cases, LVEF is reduced but not substantially (41 to 49%), though the patient still has symptoms of heart failure, which is known as HFpEF borderline. Thus EF must be considered with the volume of the heart chambers and how well they fill. In an extreme form, heart failure may result in cardiogenic shock. Shock refers to a state where there is inadequate blood flow to meet the body’s oxygen demands globally (i.e. throughout the entire body), and cardiogenic specifies that the shock is because of the heart’s failure to do its job rather than e.g. loss of fluid volume (e.g. from bleeding) or an issue of the vasculature (e.g. widespread dilation of the blood vessels causing the blood to pool in the vascular beds and not flow to the organs where it is needed). If cardiogenic shock develops, even with appropriate treatment, the survival rate is rarely above 30%.
Bennett JE, Dolin R, Blaser MJ. Mandell, Douglas, and bennett’s principles and practice of infectious diseases: 2-Volume set. 9th ed. Philadelphia, PA: Elsevier - Health Sciences Division; 2019
The electrical activity of the heart can be evaluated with an electrocardiogram (ECG, or EKG); findings are often described in terms of particular waveforms that occur on the ECG and their properties (I give sample properties in parentheses in the following non-comprehensive list) e.g. the PR interval (shortening, lengthening), QRS complex (widening, narrowing), T wave (peaked, inverted), U wave (absent), q wave (present), J point (elevation, depression) as well as the rhythm (regular, irregularly irregular). An ECG also examines the current through the heart at multiple angles via different leads (i.e. a pair of electrodes that measure current), and so when describing an ECG one has to reference the leads in which a particular phenomenon is observed. Evaluation of the mechanical function of the heart can be accomplished with imaging studies like echocardiography or cardiac magnetic resonance imaging (CMR). The function of the heart (i.e. the cardiac cycle) is summarized generally in the Wiggers diagram, for those seeking more detail.
I: Myocarditis
Definition
The term myocarditis literally means “inflammation of the myocardium,” which is the muscular, middle layer of the heart. This does not specify either a cause for the condition (etiology) or its severity (clinical spectrum). More formally, what is classically known as myocarditis is an inflammatory process of the myocardium, whose causes are elaborated upon in the next section. Myocarditis is grouped with its complications under the umbrella term of “inflammatory cardiomyopathies.” This term is often criticized for being uninformative because it does not classify the cardiomyopathy as being arrhythmogenic or dilated.
Etiology (Cause)
Inflammation itself can have many causes and so in a formal sense myocarditis may occur from ischemic damage such as with acute coronary syndrome, mechanical trauma, or from a genetic cardiomyopathy- but these would not classically be regarded as myocarditis (and in particular, it is an important diagnostic challenge to distinguish between myocarditis and acute coronary syndromes). Classically myocarditis is grouped into causes which are infectious, non-infectious, or autoimmune/immune-mediated. More granularly, Table 63-1 lists specific causes of the condition, but in most cases of infectious myocarditis a causative pathogen is not identified, and the condition is often idiopathic (i.e. cause is unknown). The etiology is a significant determinant of the severity of the myocarditis, though there are many possible causes.

Bennett JE, Dolin R, Blaser MJ. Mandell, Douglas, and bennett’s principles and practice of infectious diseases: 2-Volume set. 9th ed. Philadelphia, PA: Elsevier - Health Sciences Division; 2019
With some exceptions depending on the part of the world, viral etiologies are the most common causes for myocarditis (particularly in children). Particularly significant offenders include parvovirus B19 (this one is especially known to cause myocarditis resembling ACS), coxsackieviruses (B3 (CVB3) in particular) and other enteroviruses, adenoviruses, and human herpesvirus 6 (HHV-6). SARS-CoV-2 is also a known cause of myocarditis (discussed in II).
Of the bacterial causes, diphtheria (Corynebacterium diphtheriae) was significant in the pre-vaccine era, and the myocarditis was thought to be mediated by its exotoxin, which is cytotoxic, but the incidence of diphtheria has declined drastically thanks to vaccination; this was thought to be the most common reason for death in diphtheria, which occurred in about 5-17% of cases. Borrelia burgdorferi (the Lyme spirochete) is an important cause of endemic forms of myocarditis and in particular is associated with electrical abnormalities (high-degree atrioventricular block is the most common presentation). It should be noted though that this is a rare manifestation of Lyme disease (roughly 1.1% of cases) and resolves with antibiotic therapy.
Though there are no heritable forms of myocarditis, there are conditions which are heritable that may increase risk e.g. familial hypereosinophilia. Myocarditis may occur as a hypersensitivity (i.e. allergic reaction) induced by substances, but in some cases the substances are themselves directly toxic e.g. zinc phosphide (a rodenticide) produces phosphine gas within the body which is toxic to cardiomyocytes.
Immune checkpoint inhibitors (ICIs) are worth a specific mention as a medication which carries a risk of myocarditis. Checkpoint inhibitors are a group of immunotherapies (monoclonal antibodies) used principally in cancer where they serve to disinhibit common pathways (most work by targeting the PD-1/PD-L1 pathway or act against CTLA-4) that the immune system uses to suppress responses, thereby provoking responses against tumors and causing clearance. However, the therapies themselves can have varying degrees of specificity and potential for off-target effects. These therapies can cause a clinically severe form of myocarditis with a mortality risk of 25 to 50%. It is not entirely clear what the exact mechanism of this form of myocarditis is, but one thought is that there is crossreactivity in antigens in the tumor and the myocardium. Another thought is that PD-1 is expressed by cardiomyocytes as a safeguard against myocarditis and so an anti-PD-1 antibody suppresses this natural mechanism. ICI-related myocarditis is graded on a 4-point scale where 1 refers to only abnormal cardiac biomarkers or ECG changes and 4 describes life-threatening disease with imaging changes, symptoms, and LVEF decrease to below 50%.
Giant cell myocarditis (GCM) is a rare form of myocarditis that tends to be associated with autoimmune diseases and presents at a younger age (mean age of 42.6±12.7 years) that also tends to be more clinically severe than other forms. It commonly presents with heart failure and severe arrhythmias like high-degree heart block and ventricular tachycardia. Granulomas (aggregates of cells formed in response to inflammation that are thought to represent an ancient form of immune protection intended to “wall off” the offending threat) are present in giant cell myocarditis on histology and there is typically eosinophilic or lymphocytic infiltration. The disease is thought to be driven by autoimmune processes.
Tschöpe C, Ammirati E, Bozkurt B, et al. Myocarditis and inflammatory cardiomyopathy: current evidence and future directions. Nat. Rev. Cardiol. 2021;18(3):169–193.
Cardiac sarcoidosis (CS) is also worth mentioning as it can cause a unique form of myocarditis. Like GCM, there are also granulomas, but they typically do not have eosinophils. CS tends to be even more severe than GCM, and in patients with sarcoidosis, the condition is often a cause of death. In cardiac sarcoidosis, patients can rapidly develop heart failure and the condition generally presents initially as serious arrhythmias like atrioventricular blocks and ventricular arrhythmias. Because cardiac sarcoidosis is an autoimmune disease, the mainstay of treatment is immune suppression. It has been proposed that GCM and CS represent the same inflammatory cardiomyopathy but opposing entities of the same clinical spectrum. Fibrosis is more advanced in CS compared with GCM, while eosinophils are more likely in GCM than CS.
Not listed on the table, but still potentially important causes of myocarditis also include radiation (as in for cancer therapy), heatstroke, and even hypothermia.
Ferreira VM, Schulz-Menger J, Holmvang G, et al. Cardiovascular magnetic resonance in nonischemic myocardial inflammation: Expert recommendations. J Am Coll Cardiol 2018;72(24):3158–76
Diagnosis
A diagnosis of myocarditis in children is suspected when children develop symptoms of heart failure, typically of a short duration, as well as gastrointestinal and respiratory symptoms following an apparent viral illness. Symptoms may also include new chest pain and shortness of breath. Fever may also occur. In children respiratory symptoms can predominate. Kids will also often have a rapid heart rate, low blood pressure, lethargy, enlarged liver, and difficulty breathing when lying down. Misdiagnosis in the emergency department initially is common because of how nonspecific symptoms are. In general, because of its rarity and nonspecific presentation, there needs to be a high degree of suspicion for myocarditis. A chest x-ray may show cardiomegaly. In adults, there may be unexplained heart failure, chest pain and arrhythmias, especially following a systemic infection. Chest pain is more likely in adults than in children with myocarditis (though pericarditis does cause chest pain in children and may co-occur with myocarditis as myopericarditis). Myocarditis may also occur asymptomatically and be noted incidentally. Some sources (Fleisher and Ludwig) do consider myocarditis to be a clinical diagnosis (i.e. made on the basis of clinical presentation) but there are more robust means.
Myocarditis may also cause ECG changes and because it causes cardiac injury, cardiac troponins may leak into the blood. However, a negative troponin does not exclude a diagnosis of myocarditis, and similarly troponins may elevate for other reasons e.g. ACS. There are other biomarkers which can be used as well to help confirm myocardial injury like CK-MB and NT-pro-BNP. Troponin I (TnI) is thought to be a potential autoantigen that the immune system targets in myocarditis in addition to a biomarker, but caution is warranted as autoantibodies may be present in healthy individuals as well. The ECG changes that occur with myocarditis vary greatly depending on the cause, and there aren’t ECG changes specific to myocarditis. ST elevations diffusely may occur, but focal forms of the condition may present with more localized ST elevations. Tachyarrhythmias may occur as well, though some etiologies of the condition do cause bradyarrhythmias. A normal ECG is also not sufficient to exclude a diagnosis of myocarditis. Some ECG changes that may occur in myocarditis are also specified in Table I.
Ferreira VM, Schulz-Menger J, Holmvang G, et al. Cardiovascular magnetic resonance in nonischemic myocardial inflammation: Expert recommendations. J Am Coll Cardiol 2018;72(24):3158–76
A definitive diagnosis of myocarditis can be made only by endomyocardial biopsy (EMB). This involves taking a biopsy of the heart tissue to look for evidence of infiltration by the cells of the immune system (which is performed endovascularly, though the preferred access site varies with the location the procedure is being performed in; in some centers it has been reported that biopsying the left ventricle is as safe and has greater diagnostic yield than biopsying the right). Though this is considered the gold-standard diagnostic method for myocarditis, there are problems, and the procedure is so specialized that it is rarely done outside of specialized academic centers. The most obvious of these is that a biopsy of the heart is an incredibly invasive thing to do (complications can happen, though rare if performed by someone experienced in the procedure), and of course being a biopsy, it’s very easy to “miss” and get healthy heart tissue that doesn’t show evidence of myocarditis even if it is occurring (some forms of myocarditis can be highly focal). EMB is a very specific test but has poor sensitivity. For this reason, EMB is essentially only ever done if the case of myocarditis is very severe (it is generally thought to be most useful if GCM or fulminant lymphocytic myocarditis) and it is likely to give useful information about the condition’s treatment (and this also maximizes pre-test probability). Then comes the matter of interpretation. The standard criteria used for this are the Dallas criteria but there is a lot of variation in how the specific slides are interpreted, and some forms of the condition may appear borderline or appear to mix histological types (e.g. an EMB on a patient who developed myocarditis after the smallpox vaccine showed a lymphocytic-eosinophilic infiltration). However, in addition to Dallas criteria, PCR can be done to look for viral causes on the EMB and immunohistochemistry staining can also be done to more accurately delineate the type of myocarditis.
The final principal option for diagnosing myocarditis is through the use of imaging, either by echocardiography or cardiac MRI (CMR). Echocardiography tends to be more accessible and principally focuses on an assessment of left ventricular function, though there are no specific echocardiographic features that can diagnose myocarditis. Patients may have a spherical ventricle with reduced systolic function in the acute phase. In fulminant cases their heart chambers may appear small with mild hypertrophy caused by the inflammation. Additional pericardial inflammation may be present, indicating myopericarditis. Right ventricular dysfunction may occur but it is rarer and a poor prognostic sign. Some wall motion abnormalities suggestive of an acute myocardial infarction (heart attack) may occur. Echocardiography can also be used to assess circumferential and longitudinal strain which are predictive of the risk of future events. Imaging can be used to identify regions of the heart where inflammation is occurring and thus ensure higher sensitivity with EMB.
CMR may be less accessible but is generally considered more sensitive and diagnosis is made under the modified Lake Louise criteria. Under these criteria, evidence for myocarditis includes edema (i.e. swelling), hyperemia (engorgement of the blood vessels from too much blood inside them), necrosis, and myocardial scarring as defined by either early gadolinium (a dye used for imaging) enhancement (EGE; corresponding to increased capillary leak and hyperemia) or late gadolinium enhancement (LGE; corresponding to necrosis, fibrosis, or edema). This technique can also pick up subtle heart dysfunction that plain echocardiographic images do not pick up. The diagnosis via CMR requires establishing myocardial edema as well as evidence of nonischemic myocardial injury. It can be supported by the presence of a pericardial effusion (i.e. myopericarditis). The lesions in myocarditis are commonly patchy and subepicardial but can also be present diffusely throughout the entire myocardium if inflammation is severe enough. Ventricular dysfunction on imaging is not a sensitive nor specific finding for myocarditis, however. It’s also critical to note that the timing at which CMR is performed is critical for accurate diagnosis. Some argue that if obtained too soon in disease course, its sensitivity is reduced, and there is a general consensus that it should be done within 2 weeks of symptom onset. The Lake Louise expert group noted that a repeat CMR should be performed 1 to 2 weeks after disease onset if the initial one is nondiagnostic but there is high clinical suspicion for myocarditis. Additionally, caution is warranted in that nonischemic inflammation of the myocardium is not specific to myocarditis. PET imaging can be valuable for diagnosing cardiac sarcoidosis and its findings can be used to corroborate CMR findings but it is arguably an even more specialized imaging modality.
More recently, in pursuit of noninvasive means to diagnose myocarditis, a recent paper describes sampling for microRNAs in circulation known to be elevated during the condition with high sensitivity and specificity. The microRNA reflects the action of Th17 cells that are involved in the acute phase of myocarditis but not its potential mimics e.g. acute myocardial infarction, and so, it may be a valuable marker for myocarditis. However, this marker is not yet validated and there may be some time before it attains routine use at the bedside. The issue here though is of course even though there is high sensitivity and specificity, the positive predictive value of the test depends on the prevalence of the condition in the population, and that’s a very complex matter as the next section describes.
Epidemiology
Wu M-H, Wu E-T, Wang C-C, et al. Contemporary postnatal incidence of acquiring acute myocarditis by age 15 years and the outcomes from a nationwide birth cohort. Pediatr Crit Care Med 2017;18(12):1153–8
Myocarditis has an extremely challenging epidemiology that complicates attempts to analyze it as a vaccine-associated adverse event. To start with, myocarditis can be asymptomatic, but it is seemingly impossible to know how often this occurs because patients who are asymptomatic do not typically present for care (the exception being that they seek care for something else and myocarditis is noted incidentally, but of course this doesn’t allow for rigorous estimation of incidence). It is thought to be the third-leading cause of sudden cardiac death in young adults and is frequently found on autopsy series. However, this obviously biases towards severe presentations of myocarditis (as they are lethal, or occur alongside lethal conditions) and the condition itself is frequently mild and self-limiting, particularly when therapy is promptly initiated (at least of the cases we detect); thus it is reasonable to assume that the incidence of myocarditis is significantly underestimated. This naturally makes comparisons to a background rate of the condition to determine excess cases challenging. A commonly cited value is 10 to 22 cases per 100,000 people per year; however this typically refers specifically to viral myocarditis. Viruses are the most common etiologic agents for the condition (although this does depend on where you are in the world; in South and Central America, Chagas disease is the most common cause) but not the only one, and thus this value, at least its lower bound, likely represents an underestimate. Fung et al report approximately 22 per 100,000 cases per year. Again though, the burden of subclinical myocarditis is not known, and the clinical importance of the condition is debated. Additionally, as previously discussed, there are many conditions which can resemble myocarditis clinically, potentially resulting in misdiagnosis that reduces the number of documented cases. Because the background rate of the condition is not well established, it is hard to gauge to what extent vaccine-associated cases represent a risk increase, and furthermore how the severity of the condition compares to “typical” cases (is a case of myocarditis requiring hospitalization and advanced therapy typical? We can’t really say for sure). The general trend seems to be towards increasing incidence, but this is further complicated in light of the pandemic, as viruses, being the most common cause of the condition, had significant changes to their incidence as a result of various pandemic control measures.
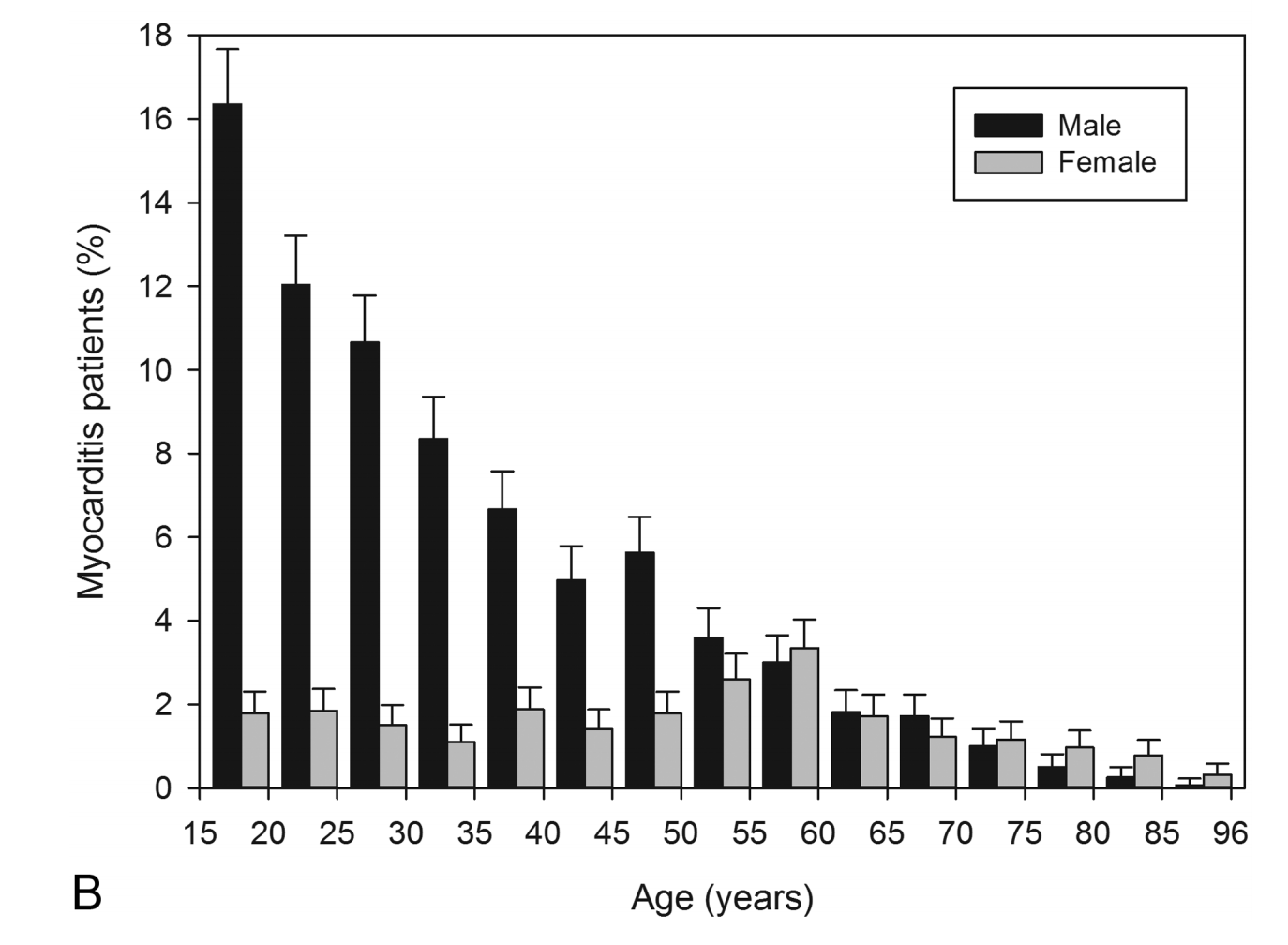
Kytö V, Sipilä J, Rautava P. The effects of gender and age on occurrence of clinically suspected myocarditis in adulthood. Heart 2013;99(22):1681–4.
A further challenge in establishing the background rates comes from limitations in the ability to diagnose myocarditis. A formal diagnosis absolutely requires an EMB, but, as above, this test is so invasive that it is generally not performed unless the patient is very seriously ill and the test has poor sensitivity: It’s easy enough to biopsy a part of the heart which does not exhibit leukocytic infiltration when there is a myocarditis at play. Furthermore, there is a high degree of inter-observer variability when analyzing slides according to the Dallas criteria (and for that reason there have been additional criteria added like immunohistochemistry and PCR).
The burden of myocarditis varies with age; Vasudeva et al estimated 0.8 cases per 100,000 children per year between 2007 and 2016 in the US. Wu et al. used a nationwide birth cohort study from Taiwan and found a cumulative incidence of 0.45 per 1000 children under age 15 from 2000 to 2014 (annual incidence ≈ 3.2 cases per 100,000 children per year assuming burden each year was equal); however these results might not generalize to other populations because of the different causes of myocarditis having unequal geographic spread. As per Wu et al, the risk peaks at the first year of life and subsequently declines until approximately puberty. Mortality from the condition was significant, cumulatively 6.2% among this cohort of 2.1 million children (965 cases with 61 deaths). Nonetheless, this does reinforce that myocarditis is likely more common than commonly appreciated. As per Kyto et al, the incidence of the condition overall appears to peak at about 15 and declines gradually.
Myocarditis is also subject to sex biases. There is a general consensus in the literature that myocarditis has a male sex bias (about 3.5:1 males to females), attributed commonly to cardioprotective factors present in women at higher levels, as well as the effects of testosterone on immunological factors like TLR4 expression and MAVS signaling. Some argue that the estrogens present in women promote an immunoregulatory response within the heart that suppresses further damage and progression of the myocarditis, and testosterone experimentally is shown to enhance viral replication in myocarditis. This is notably at odds with autoimmune diseases generally which skew strongly towards women, though myocarditis does have autoimmune components (see “Pathophysiology and Clinical Spectrum” section). Female patients tend to have more severe symptoms on presenting for care than men and are more likely to develop diastolic heart failure, but men are more likely to develop systolic heart failure. Importantly, sex bias was minimal in the Wu et al cohort study, and in a Finnish cohort, sex disparities are not apparent until about six years of age (though importantly these features may not generalize to other populations so they should be interpreted with caution). As per Kyto et al, the sex biases appear to peak at approximately 15 years of age, and then stabilize over time. In this same study, it was found that 85% of cases were idiopathic, though of the cases with known etiologies, viruses were the most common (5%). In this same study, women were noted to have a higher frequency of ventricular arrhythmias, and their duration of hospital stay tended to be longer, with a median of 5 days across the entire cohort of 3198 patients. This study did also use a Finnish cohort however, so caution is needed in generalizing these findings to other populations.
The seasonality of myocarditis is a bit controversial. Many of the viruses that cause myocarditis are highly seasonal, so it would naturally be expected that myocarditis peaks alongside these viruses, and there is some evidence for this. On the other hand, other studies show a minimal seasonal effect. Obviously, seasonality would be subject to the specific location in the world as the agents causing myocarditis have variable endemicity. However, the mitigation measures taken against COVID-19 have caused profound changes in the incidences of a number of respiratory viral infectious diseases, and as these measures are being relaxed, many of these viruses are showing a resurgence out-of-season. This further makes it very complicated to disentangle the possible causes of myocarditis in these patients as some cases may be the coincidental result of a different viral infection.
Pathophysiology and Clinical Spectrum
Figure 3. Ammirati E, Veronese G, Bottiroli M, et al. Update on acute myocarditis. Trends Cardiovasc. Med. [electronic article]. 2020;(http://dx.doi.org/10.1016/j.tcm.2020.05.008)
Myocarditis has a lot of variation in how it presents and how its various causes produce disease. For instance, despite requiring inflammation from the myocardium, most infectious agents shown to cause myocarditis have not demonstrated cardiac tropism in vivo with the notable exceptions of Trypanosoma cruzi, enteroviruses, and adenoviruses (SARS-CoV-2 has also demonstrated cardiac tropism). However, it is thought that cardiac tropism is dispensable for the induction of myocarditis as some viruses appear capable of causing immunological derangement sufficient to produce the syndrome (see table 1 Tschope et al, 2020). In the clinical sense, myocarditis has three possible phenotypes (in order of frequency):
Caforio ALP, editor. Myocarditis: Pathogenesis, Diagnosis and Treatment. 1st ed. Cham, Switzerland: Springer Nature; 2020
Acute myocarditis is the most common form wherein patients may have nonspecific cardiac symptoms e.g. fatigue, shortness of breath, chest pain, arrhythmias, and palpitations, and the most common outcome is resolution. It usually occurs following an upper respiratory or gastrointestinal infection.
Fulminant myocarditis (about 10% of biopsy-proven cases as per Braunwald; in the Marburg Myocarditis Registry of 1000 patients with biopsy-confirmed myocarditis only 2.5% presented with the fulminant phenotype, but in other studies the prevalence was as high as 30%. This phenotype is reliably considered rare, however) presents with rapid cardiac decompensation manifest by arrhythmias and hemodynamic derangements (often requiring pressor support) secondary to severe myocardial inflammation. This typically occurs suddenly with progressive worsening over 2 weeks but potentially as quickly as 2-3 days. Often pressor support is inadequate to maintain blood pressure and mechanical circulation support (MCS) devices are required. This form of myocarditis may occur in those who are severely immunocompromised, those with poorly controlled autoimmune disease (e.g. lupus, scleroderma, Sjogren’s), those on checkpoint inhibitor therapy, and other patients. Cytokines are often dramatically elevated in fulminant myocarditis. Histologically, this form may be lymphocytic (usually in viral forms), eosinophilic (usually as a hypersensitivity reaction to a drug), or giant cell (usually due to an underlying autoimmune disease). ICI-related myocarditis usually presents as a fulminant myocarditis.
Chronic active myocarditis represents a persistent form of myocarditis where there is constant, low-grade inflammation after an initial acute myocarditis, with resultant potential for arrhythmias, heart failure, and progression to DCM. Intramural and epicardial scarring may also occur.
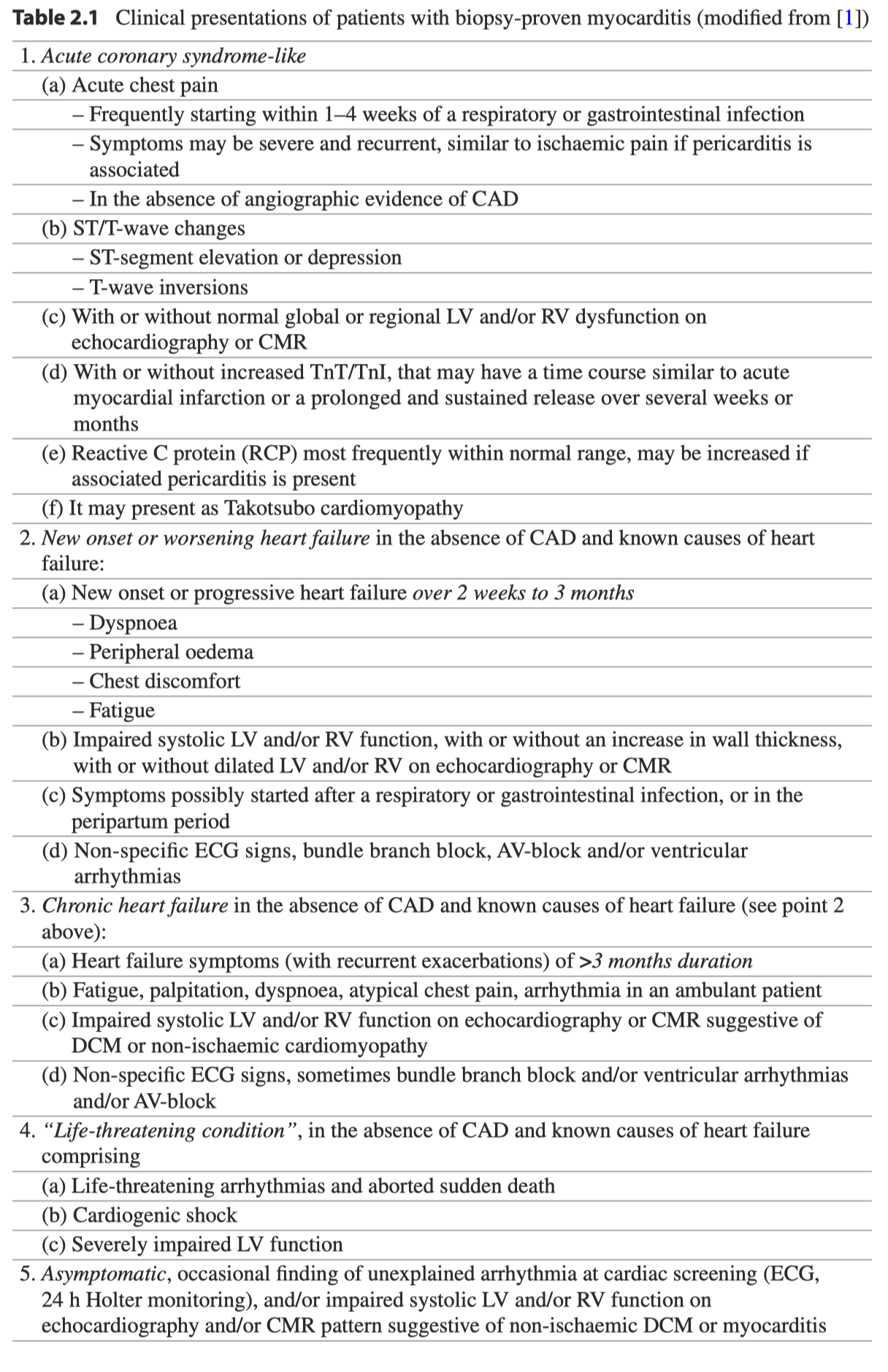
Other sources classify the condition more granularly (see table 2.1).

Caforio ALP, editor. Myocarditis: Pathogenesis, Diagnosis and Treatment. 1st ed. Cham, Switzerland: Springer Nature; 2020
For simplicity, I will focus on the 3-category system. The condition may present differently depending on the patient’s age: younger individuals may have more pronounced inflammatory responses to the initial infectious trigger of the myocarditis, while in older individuals there is a greater tolerance to inflammation and they may present later in the clinical course. Thus acute and fulminant presentations are more common in the young. Failure to resolve the myocarditis results in progression to heart failure, dilated cardiomyopathy (DCM), and eventually death or heart transplantation. It is worth explaining DCM a bit more. DCM is a condition in which the chambers of the heart (usually the left ventricle but sometimes the right as well) become dilated (as the name suggests) and unable to adequately contract to circulate blood, producing heart failure. DCM is thought to represent in many cases a complication of myocarditis that is not properly resolved and thus for that reason is regarded by some experts to be among its more extreme manifestations (and thus anything that causes myocarditis can potentially cause DCM), though there are genetic causes for the condition (note that there are no genetic conditions which can directly cause myocarditis but there are some which increase risk). Most commonly the condition either has no identified cause in the given patient or appears to be the result of pathologic genetic variants. DCM is largely the result of the accumulation of scar tissue in the myocardium that prevents adequate contractions, causing a decline in cardiac output that results in heart failure. To compensate for this, pressure in the veins increases and the arteries become stiffer, causing an increase in both preload and afterload. This disrupts the ability of the heart chambers to fill during diastole (relaxation) and increases stress on the walls of the heart. What’s more is that DCM can be slow to show symptoms and by the time patients present for care it is often too late to meaningfully intervene. DCM does have multiple options for its management depending on the cause as there are medical therapies and devices to treat heart failure and exercise is shown to be beneficial for these patients, the only definitive treatment for it is heart transplantation (and cardiac transplant brings with it a separate set of challenges related to immunosuppression, and there are limited data on how these patients fare long-term).
In short, myocarditis may range from an apparently asymptomatic condition that self-resolves to causing decompensated heart failure and sudden cardiac death, or DCM requiring transplant.
Coxsackievirus (CVB3) myocarditis is the most common reference for viral myocarditis as this is what most rodent models are based on; it progresses through stereotyped phases. The initial infection generally progresses as an uncomplicated febrile illness, and the clinical spectrum of CVB3 myocarditis can span from asymptomatic disease to sudden cardiac death (the clinical spectrum of acute myocarditis is summarized in Figure 3).
Heymans S, Eriksson U, Lehtonen J, et al. The quest for new approaches in myocarditis and inflammatory cardiomyopathy. J. Am. Coll. Cardiol. 2016;68(21):2348–2364
In a mouse model of CVB3 myocarditis, there is a stereotyped sequence of cytokines which results in progression from viral to autoimmune myocarditis and then to DCM. Broadly, there is initially inflammasome activation and release of TNF-α, which is followed by type 2 inflammation as a compensatory response. Eosinophilic infiltration may follow and there is downregulation of the immunoregulatory cytokine IL-10. As the autoimmune myocarditis progresses, there is a shift to type 17-driven inflammation that causes progression to DCM. IL-17A is required for progression to DCM.
Rose NR. Critical cytokine pathways to cardiac inflammation. J. Interferon Cytokine Res. 2011;31(10):705–710
This resource is strongly recommended for anyone interested in the cytokine pathways driving myocarditis and its various phases.
Phase 1 (Viral Infection, aka acute stage): This phase involves the initial invasion of the virus into cardiomyocytes, causing innate immune activation, and lasts for up to 1 week. In the case of CVB3, there is an initial binding step to decay-accelerating factor (DAF) which results in subsequent entry via the coxsackie-adenovirus receptor (CAR) located at the intercalated discs of the cardiomyocytes (i.e. cell-cell junctions). CAR is the receptor for the virus and its ablation abrogates infection. The virus replicates on autophagosomes with the aid of miRNA to enhance replication. Replication within the cells is cytotoxic, and results in death of the infected cardiomyocyte with liberation of DAMPs and production of pro-inflammatory cytokines. Dissemination of coxsackievirus is aided by protease 2A which cleaves dystrophin to reduce the integrity of the sarcolemma (and in so doing directly contributes to the development of cardiomyopathy) and permit viral egress.
As this occurs, the cardiomyocyte begins to secrete type 1 interferons in response to the infection and this is generally sufficient to substantially restrict viral replication, seemingly through both a MAVS-dependent pathway mediated by RNA helicases, MyD88, and IRAKs via TLRs. TLR3 knockout mice have very high mortality from enteroviral myocarditides and TLR3 polymorphisms have been associated with myocarditis in humans. A fulminant myocarditis occurs in mouse models exhibiting interferon deficiency, and interferon deficiency is associated with progression to DCM. TLR4-driven inflammation is also associated with poorer outcomes and CVB3 upregulates TLR4. Experimentally, the addition of LPS (a TLR4 ligand) in mice with myocarditis results in fatality to 70% of them by day 15 with much more severe inflammatory changes within the heart.Phase 2 (Autoimmunity, aka subacute stage): Following a period of sensing and activation, the inflammation results in recruitment of several key cell types, initially NK cells (as well as iNKT cells and γδ T cells) which are followed by macrophages and then T cells, with T cell infiltration peaking at 7 to 14 days. These promote clearance of the virus, which can be sufficient for resolution of the myocarditis over a period of 1-4 weeks. More rarely, there is progression to the next phase of the condition. This stage of the myocarditis can result in substantial tissue damage to the myocardium, however. Cytotoxic T cell levels correlate with the extent of myocardial damage, but the evidence on whether or not T cell depletion is valuable in the setting of myocarditis is mixed. Earlier literature had reported that depletion of either CD4 or CD8 T cells improved outcomes in CVB3 myocarditis, but in SCID, myocarditis has been shown to be fulminant (however the SCID phenotype in question also causes an absence of B cells). Progression to autoimmune disease is promoted in genetically resistant mice with TNF-α or IL-1. Regulatory T cells restrict tissue damage through upregulation of IL-10 and TGF-β and prevent autoimmune disease. Sequelae are likely if there is inadequate responsiveness from regulatory T cells. IL-4, a prototypical type 2 cytokine, has a very strong association with the severity of myocarditis and its inhibition improved outcomes and was associated with enhanced production of type 2 interferon; thus it is thought that IL-4 inhibits production of type 2 interferon and promotes severe disease. Interestingly, IL-13, another type 2 cytokine associated with anaphylactic antibodies, appears to limit the extent of fibrosis and inflammation. IL-17 is thought to promote prolonged inflammation that may lead to the development of autoantibodies. Cardiac myosin is a key target of autoantibodies, and when altered appears to be capable of serving as a ligand for TLR4.
Phase 3 (DCM, aka chronic stage): There is a branching of the pathways herein: (1) Left ventricular function may normalize if clearance of the virus is successful and no post-viral/autoimmune sequelae result.
(2) Alternatively, in a minority of patients there is persistence of the virus resulting in continued tissue damage, chronic inflammation, and progression to DCM. As a consequence of the persistent damage from the chronic inflammatory stages, the myocardium may undergo fibrotic changes that compromise its pump action. There are hints of a genetic correlation in association with the outcome of this third phase. It is thought that in some cases, CVB3 infection results in bystander activation sufficient to provide requisite costimulation to autoreactive lymphocytes and generate autoimmune reactions directed against the heart. There is evidence of cross-reactivity between antibodies targeting CVB3 antigens and group A streptococci (GAS; the causative agent behind rheumatic fever) antigens wherein the antibodies appear to neutralize CVB3. Alternatively, there is evidence of viral persistence in those cases which progress to DCM by PCR; however this has been questioned because these RNA sequences have also been found in control patients. It is probable that both viral persistence and epitope spreading with bystander activation play roles in the pathogenesis of viral myocarditis-induced DCM.
Progression to (2) appears to be related to a shift in cytokine profile towards Th17 skew is associated with autoimmune progression of the myocarditis that eventually culminates in DCM and fibrosis and drives chronic inflammatory myocarditis (phase 3). IL-17 and IL-23 appear to be key cytokines in this process. IL-23 is required for the development of experimental autoimmune myocarditis and IL-17 is required for myocardial fibrosis and chronic inflammatory changes which result in progression to heart failure and fatality. Mechanisms thought to underlie this include suppression of IL-6 production during the third week (IL-6 enhances myocardial contractility) and enhanced inhibition of matrix metalloproteinases (MMP) 2 and 9 required for cardiac remodeling. Knockout of IL-17A is sufficient to prevent progression into heart failure that is eventually fatal. IL-22 on the other hand appears to be protective in viral myocarditis, and Th22 cells may therefore play a protective role as well, but this has not yet been validated experimentally.
It is worth mentioning that if DCM occurs, it is hard to tell whether or not it is because of myocarditis progressing into it or because it was already present and the patient’s clinical deterioration made it clinically apparent.
The development of myocarditis in mice appears related strongly to genetic susceptibility as in mice with CVB3-induced myocarditis, by about day 9, no viral replication was noted and symptoms had resolved in the mice. The mice whose symptoms persisted after day 9 demonstrated cardiac autoantibodies and autoimmune disease. This observation is used to establish an experimental autoimmune myocarditis model. Adoptive transfer studies of mice with CD4 T cells from those with autoimmune myocarditis reproduces the disease in mice which are healthy. Mice lacking the IL-12 receptor proved resistant to myocarditis; however, knockout of the STAT4 protein involved in signaling downstream of IL-12 resulted in an eosinophilic infiltration of the myocardium. IL-12 is thought not to be required for myocarditis but its deficiency is associated with enhanced viral replication, thought to be from depletion of neutrophils and macrophages. Type 2 interferon has been shown to be protective in autoimmune myocarditis, seemingly through the induction of apoptosis in CD4 T cells that drive the disease. Mice lacking IL-13 showed a much higher likelihood of progression into DCM and died of heart failure. IL-13 may inhibit type 1 inflammation and inflammasome activation that occurs earlier in this stage, as mice lacking it had much higher levels of IL-1β and IL-18 (type 1 cytokines released through pyroptosis).
Another well characterized virus known for causing myocarditis is parvovirus B19 (B19V). B19V is able to establish a persistent infection within the bone marrow in childhood (as its primary infected cell is the erythroid progenitor) and subsequently can infect endothelial cells, including those in the heart, but does not replicate within cardiac endothelial cells; following this it can induce production of pro-inflammatory cytokines like IL-6 and TNF-α and trigger apoptosis of the cardiomyocytes. Like CVB3, the severity of B19V myocarditis spans the entire clinical spectrum of the syndrome. EMB generally demonstrates lymphocytic infiltration but myocyte necrosis may be absent and damage may be inapparent. B19V antigens have also demonstrated antibody crossreactivity with human autoantigens.
Ong S, Rose NR, Čiháková D. Natural killer cells in inflammatory heart disease. Clinical Immunology. 2017;175:26–33.
Several immune cell types are particularly important to the pathogenesis of myocarditis. Natural killer (NK) cells are critical for controlling the extent of myocarditis, especially viral myocarditis. NK cells recognize missing self and altered self signals and mediate viral clearance early in the course of infection, thereby preventing viral persistence that is important in some progression to DCM, and are an important source of type 2 interferons. This serves to both suppress signals from ILC2 cells which, though rare, are prolific sources of type 2 cytokines that are associated with poorer prognosis in myocarditis and recruitment of eosinophils to the heart (eosinophilic myocarditides tend to be more severe compared to other forms); depletion of NK cells enhanced eosinophil recruitment. Type 2 interferons also induce apoptosis of eosinophils, and promote maturation of monocytes. NK cells also inhibit fibrosis, which is especially important for progression to DCM. Viral and idiopathic forms of myocarditis in humans often present with significant NK cell deficiency.
Another key cell type that should be noted is the eosinophil. Eosinophils are key effectors of type 2 inflammation and indispensable for defense against parasites such as helminths, but are associated with a severe form of myocarditis (eosinophilia generally is associated with cardiomyopathies, and hypereosinophilic syndromes are associated with cardiac complications in ~20 to 50% of cases). Eosinophilic myocarditis may occur as a manifestation of a hypersensitivity reaction e.g. DRESS (drug-related eosinophilia with systemic symptoms) syndrome. Peripheral eosinophilia is also noted in most (90%) cases of hypersensitivity myocarditis in a case series of hypersensitivity myocarditis post-heart transplant, but because multiple underlying pathologies can cause eosinophilic myocarditis, the frequency of peripheral eosinophilia varies with the cause (though in most cases does tend to be elevated). Eosinophils are an important source of IL-4, a prototypical type 2 cytokine, and in mice its knockout is sufficient to prevent progression to DCM. IL-5, another type 2 cytokine, promotes eosinophil production and survival, and in models where it is overexpressed, eosinophilic myocarditis develops and is associated with more pronounced reductions to ejection fraction, though IL-5 is dispensable for eosinophilic myocarditis; in a case report, anti-IL-5 antibody therapy was associated with clinical improvement of a patient with eosinophilic myocarditis. Thus eosinophils are a key driver of progression to DCM. Notably, though the myocardium may fibrose in eosinophil-driven forms of myocarditis, there is not always a reduction in ejection fraction. Major basic protein, the most abundant protein in eosinophilic granules, promotes vascular thromboembolism in patients with eosinophilic myocarditis. Eosinophils appear to primarily affect cardiac remodeling to induce DCM. It is noteworthy that both Th17 cell-mediated inflammation and eosinophil-driven inflammation both appear to drive progression to DCM. One possible explanation is that Th17-derived GM-CSF promotes eosinophilopoeisis and promotes their survival, thus suggesting a pathologic synergy; it has been suggested before that eosinophils play an underappreciated role in Th17-driven inflammation. When the cause is hypersensitivity, especially to a drug, patients tend to improve markedly upon its discontinuation.

Peretto G, Sala S, Rizzo S, et al. Arrhythmias in myocarditis: State of the art. Heart Rhythm. 2019;16(5):793–801
The outcome of these processes is summarized pathophysiologically: myocardial contractility decreases secondary to the increase in interstitial volume associated with the inflammatory changes, which also results in edema. End-diastolic ventricular volume (EDV) also decreases because of the reduced contractility. Because of the reduced contractility, Starling forces are unable to compensate for the increased EDV, which results in reduced cardiac output. However, shock may not occur because of sympathetic effects on the vasculature (vasoconstriction to shunt blood towards vital organs and away from extremities) and compensatory tachycardia.
Electrical abnormalities may also be present and vary in frequency and severity depending on the underlying cause; giant cell myocarditis more commonly produces ventricular arrhythmias and heart block for example. Lymphocytic myocarditis tends to be more focal and thus ECG changes may be represented accordingly. Perretto et al provide a very thorough discussion of the arrhythmias that may occur in myocarditis. Most of the arrhythmias that occur in myocarditis are tachyarrhythmias (fast heart rate) except for those caused by cardiac sarcoidosis, giant cell myocarditis and the antecedent autoimmune diseases, and Chagas disease. In these latter cases, atrioventricular block may occur. B. burgdorferi and diphtheria can cause ventricular arrhythmias and acute phase atrioventricular block, as can Chagas disease. The arrhythmias are thought to result from any of the following:
Cytopathic effects causing electrical instability of myocytes
ischemia as with endothelial-tropic viruses like B19V
gap junction dysfunction from impaired connexon expression as seen in CVB3 infection
derangements in calcium currents
Alternatively, granulomas may contribute to giant cell and cardiac sarcoidosis or other autoimmune diseases.
Prognosis of arrhythmias in myocarditis varies. For fulminant myocarditis there may be short-term ventricular arrhythmias which are life threatening, and fatal arrhythmias are known to occur in giant cell myocarditis. However, arrhythmias during the acute phase are generally self-limiting and not concerning. During the acute phase of myocarditis, physical activity is associated with an increased risk of sudden cardiac death.
Arrhythmias may also occur as so-called “cold-phase arrhythmias” resulting from chronic and prior myocarditis that does not fully heal. This typically occurs if there is left ventricular dysfunction after the acute and postacute periods. The arrhythmias appear to be from ongoing inflammation (as in chronic active myocarditis) or post-inflammatory scarring. Physical activity appears beneficial for these patients, in contrast to in acute myocarditis. If this occurs, evolution of the condition to DCM is more probable. In cardiac sarcoidosis the risk can be especially high; sarcoidosis and indeed other subtypes of myocarditis have been known to affect the conduction system and cause heart rhythms that are too slow..
Treatment
Principally myocarditis is treated through supportive therapy and activity restriction; AHA and ACC guidelines for myocarditis recommend activity restriction for 3 to 6 months following diagnosis based on evidence that exercise is associated with an increased risk of sudden cardiac death in myocarditis. Reassessment for athletes is recommended every few years, and they are considered safe to return to their sport if a 24-hour Holter monitor demonstrates no concerning ECG changes and their LV function has normalized. Otherwise the management of myocarditis is based on the specific problems that arise from it e.g. inotropic support with pharmacotherapy or in extreme cases mechanical circulatory devices, diuretics to reduce myocardial edema, and antiarrhythmic medication as needed or pacemaker placement. Mechanical circulatory support may be needed in the event of severe heart failure or cardiogenic shock e.g. ECMO and VADs. Limited data suggests a positive effect of both ACE inhibitors and ARBs, as well as aldosterone receptor blockers. The use of NSAIDs is generally not recommended in myocarditis as in experimental models of viral myocarditis in mice, they generally appear to worsen things; however, more recent data (though case-controlled) suggests NSAID use may be safe in acute myocarditis with intact LVEF, but prospective, randomized data are needed to confirm. A murine study noted that Th17 inflammation that is associated with worse outcomes in myocarditis appears to act in part by the induction of COX-2 and production of PGE2, and this process is directly inhibited by NSAIDs.
A limiting factor in guiding therapy is that myocarditis is often idiopathic and EMB is rare; by determining the type of myocarditis EMB can help to determine best treatment. Giant cell myocarditis generally requires intense immunosuppression with cyclosporine and corticosteroids, and immunosuppression is also critical in management of eosinophilic myocarditis. However, if the myocarditis is because of an infectious process immunosuppression in this manner can make things much worse, and viruses are the most common cause globally; persistent viral infection results in progression to DCM. Antiviral therapies may have use in viral myocarditis, and the viruses may often persist beyond the acute phase meaning there is an adequate window of time where they may be effective. Type 1 interferons have shown utility in vitro against CVB3 myocarditis, and in small studies IFN-β shows excellent efficacy against adenoviral and enteroviral etiologies; specific antivirals can be used for other agents if they are known to be the cause e.g. ganciclovir for HHV-6 myocarditis. Intravenous immunoglobulin (IVIG) is also among the most common immunomodulatory therapies for acute myocarditis and in meta-analyses appears to improve relevant clinical outcomes including in-hospital mortality and LVEF; the mechanism for how IVIG works is incompletely understood but is believed to be related to a direct antiviral effect (i.e. from neutralizing antibodies) and an anti-inflammatory effect (this is not as well understood and typically occurs with higher doses of IVIG). In some cases, heart transplant may be required for management of myocarditis, and death following transplant is usually the result of rejection, hypothesized to be from persistence of the factors driving the initial case of myocarditis.
Prognosis
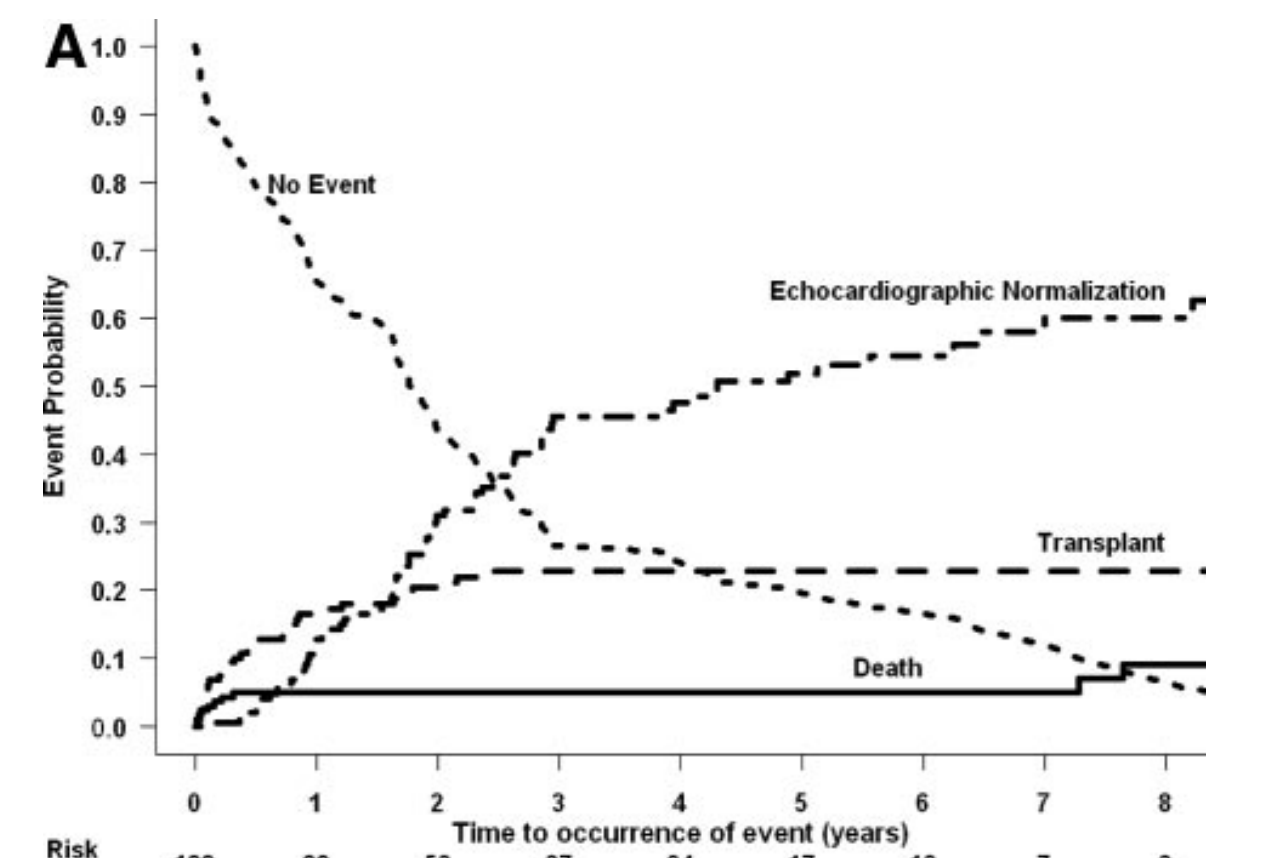
Foerster SR, Canter CE, Cinar A, et al. Ventricular remodeling and survival are more favorable for myocarditis than for idiopathic dilated cardiomyopathy in childhood: an outcomes study from the Pediatric Cardiomyopathy Registry. Circ Heart Fail 2010;3(6):689–97. Figure 2A
Most commonly, provided that there is no or minimal left ventricular dysfunction, myocarditis resolves completely. In more rare cases, fulminant courses may occur, and in a minority of cases, a chronic form of myocarditis may evolve. The condition may be complicated by progression into dilated cardiomyopathy (DCM), which may require heart transplant as a definitive treatment with circulatory support (both pharmacologic and mechanical) as a bridge to transplant. Uncomplicated myocarditis has no associated cardiac mortality and does not require transplantation. Ventricular arrhythmias from fulminant myocarditis acutely can be fatal, and high-degree atrioventricular blocks are also poor prognostic signs. Other arrhythmias are generally regarded as being less concerning. Butta et al. report that ST elevation with early repolarization indicated a better prognosis. Q waves and widening of the QRS beyond 120 ms is associated with an increased risk of sudden cardiac death. Arrhythmias occurring after apparent recovery or in the setting of chronic active myocarditis indicate an increased likelihood of progression to dilated cardiomyopathy. Higher levels of troponin, interleukin-10, and soluble Fas in the plasma are associated with a poorer prognosis. Right ventricular dysfunction on echocardiography is a poor prognostic sign. One other biomarker currently being explored is sST2 which has been associated with progression to heart failure among males ≤ 50 years old.
Among pediatric patients, Foerster et al. describe the course of a cohort of biopsy-confirmed myocarditis (n=119) or with probable myocarditis diagnosed clinically or by biopsy alone (n=253) and their outcomes together are summarized in Figure 2A. The most common occurrence over time is echocardiographic normalization, with a relative minority of cases having died and requiring transplant. LV fractional shortening was found to be inversely related to mortality, LV posterior wall thickness was directly related to transplantation. Among those with decreased LV shortening on presentation, normalization was more likely among those with greater septal wall thickness and those without LV dilation. Outcomes were similar among the group with biopsy confirmed and probable myocarditis. Among children, 4-7% of cases of acute myocarditis are fatal, and 4-9% require transplantation. In fulminant myocarditis among children, higher creatinine, lactate, and AST correlate with in-hospital mortality. LGE on CMR can be indicative of myocardial scarring, and may be present persistently even in subclinical cases of myocarditis, but scarring can recede over time. A recent cohort of pediatric patients with biopsy-confirmed myocarditis (n = 22, so caution is absolutely warranted and design is retrospective) showed that among those who had ST elevations on ECG, lower NYHA class, lower NT-BNP, fevers at initial presentation, chest pain, and higher (i.e. borderline to normal) LVEF progression to dilated cardiomyopathy was less likely occur. In this same cohort, mechanical circulatory device use, dyspnea, heart failure and inotropic medication use, decompensation, was associated with progression to DCM. Notably, these findings may also have been present in cases of myocarditis that did not progress to DCM as well.
Recurrence of myocarditis occurs in about 15% of cases.
II: Myocarditis associated with COVID-19 Vaccines and the Risk-Benefit Analysis


Undeniably, there is much uncertainty here, and in such situations, it is generally most fruitful to consider the available body of evidence and course correct as needed when more evidence emerges. I understand that to some the characterization of the vaccine-associated cases as mild sounds ridiculous because myocarditis is such a potentially serious condition (and I say potentially largely because we don’t fully understand the burden of all cases and thus don’t know how often it isn’t serious), but compared to how bad the condition can be in its “classic” forms (as discussed above- the potential for dangerous arrhythmias and sudden cardiac death, progression to heart failure, i.e. fulminant myocarditis), I don’t think it’s an unfair qualifier. While it’s true that most cases of myocarditis following the vaccines are being hospitalized, this is not typically because patients are so ill as to need hospitalization or ICU admission but rather because they need close cardiac monitoring, as explained in the CDC/IDSA clinician call on the matter. In most cases the duration of hospitalization is also shorter and patients are being discharged with over-the-counter NSAID medication. That isn’t to say uniformly that none of these patients are seriously ill, but those cases do represent outliers. Even in Israel, where the condition was first detected and reported to be as common as 1-2 cases per 6000 males aged 16 to 24, 95% of cases were classified as mild and the country is now encouraging vaccination of those 12 to 15 years old given the risks from the delta variant. I do also want to note though that even for mild cases, the management of myocarditis can be quite disruptive to daily life and quality of life because as per AHA guidelines, physical activity should be restricted for 3 to 6 months following the diagnosis as intense physical exertion is associated with sudden cardiac death (this makes me wonder whether Israel may have reported such a high incidence of the condition in part because of the vaccinees also undergoing military training -given their age- and thus more symptomatic but that is only speculation on my part and I have no evidence for that claim so it should be treated as such). The picture we have so far for these cases is largely reassuring, but there are asterisks.
The biggest caveat here is that it’s not totally clear how the condition will affect those who suffer from it over time (Such work is currently being performed by the Society of Cardiovascular Magnetic Resonance Imaging). Scarring of the myocardium in myocarditis can precipitate arrhythmias in the future, and a history of myocarditis does raise the risk of a number of cardiovascular problems significantly (for instance, mutations in the TTN gene encoding titin are common and have profound effects on cardiovascular risk, such as for the development of dilated cardiomyopathy). In this respect though, my concerns are mitigated by some immunological data. Firstly, the principal cell type found to be elevated is the natural killer cell, which is known to be protective in viral myocarditis as discussed above. Though under the assumption that these cases are caused directly by the vaccine, this is not a viral myocarditis, the mechanisms by which this occurs are not simply from enhanced viral clearance by the NK cell but because NK cells suppress both autoreactive T cells and eosinophils, which are critical in driving progression to the autoimmune and fibrotic phases of myocarditis respectively that are associated with progression to dilated cardiomyopathy and heart failure. IL-5 is also increased and this is a key cytokine involved in activation of eosinophils, but there is no peripheral eosinophilia noted in these patients as would be expected in an eosinophil-driven form of the myocarditis (which tend to be more severe), which is heartening (pun not intended). There is also heightened expression of IL-1RA which suppresses the action of IL-1β, suggesting a compensatory response against inflammasome activation that is important in the early stages of initiating myocarditis, which makes me think that the condition is in most cases abortive (and as far as we can tell that is what the data show). The problem here of course is that this data is based on a single patient and his results may not generalize to every case of myocarditis observed, so I would like to see additional immunological profiling as well as studies of the genetic factors that could be involved here. I think that obtaining an endomyocardial biopsy of a patient with this myocarditis could contribute very valuable information but almost no patients are ill enough to justify that intervention and those who are may have a form of the disease that is different from the commonly occurring ones. Additionally, based on the symptom profile of cases, most exhibited signs and symptoms that have been inversely associated with progression to DCM (chest pain, ST-T wave changes; imaging changes were rare and dyspnea was also rare).
I do also want to point out that though VAERS is a passive surveillance system and may underreport, there are biases which can cause it to give erroneously high signals as well, and underreporting is much less likely to be an issue for more serious conditions (like the kind that you get hospitalized for e.g. myocarditis). It’s important to bear in mind that it is not just the risk of myocarditis that matters but the risk increase- how many additional cases of the condition we may expect to see after vaccination. As discussed earlier, without knowing the background rate of the condition, it’s very difficult to gauge how much of a risk increase this represents, and in an absolute sense the condition is still quite rare. Additionally, just because this myocarditis is symptomatic does not necessarily mean it is more serious than subclinical forms of the condition, which are likely to be missed (myocarditis is known to cause dilated cardiomyopathy and many cases of the latter are idiopathic- potentially reflecting a case of myocarditis that progressed and was never detected which can readily happen if it does not cause symptoms; myocarditis is also a common autopsy finding among those with sudden cardiac death, which may reflect that some of those patients do not perceive symptoms from myocarditis). We are additionally seeing a resurgence in many of the viruses known to cause myocarditis presently, and thus it’s possible some of the cases of myocarditis being reported are coincidental. Note that cases due to these viruses would be essentially impossible to prove without a biopsy and that is rarely done. Additionally, by issuing an alert to look for myocarditis to healthcare providers, it’s easy to overdiagnose as the condition has many mimics. This would also hold true for other surveillance systems like the Vaccine Safety Datalink (VSD). I bring this up because any numbers we have now need to be interpreted with great caution. Underreporting is certainly possible, but there are a number of factors here that could also bias towards an overestimation of the risk and risk increase (at least, relative to our reference data). For instance, imagine the following scenario: a child gets dose 2 of the Pfizer/BioNTech vaccine and is struggling with reactogenicity symptoms e.g. fever, fatigue, headache. Parents decide to take the child to urgent care or the ER, where an ECG is performed and it shows abnormalities. Blood is also drawn showing troponin elevation. A diagnosis of myocarditis is made. Is it legitimate? Entirely possible. But we can also observe elevations in markers of cardiac injury in acute viral illnesses as well as ECG abnormalities, and this has been shown for influenza- but those tests aren’t routinely done in those circumstances. This really limits our ability to make reliable estimates of the risk increase here. The condition could be far more common than we realize and we’re just noticing it with the vaccines because of the reactogenicity symptoms associated with it. It is also far too early for us to know whether or not the event is triggered by the vaccine (in which case it does not contribute to excess cases of myocarditis but simply causes them to appear earlier) or caused by the vaccine (in which case it does contribute to excess cases), and while that may seem like an immaterial matter for the bedside, it matters a great deal. If we elect to withhold the vaccine for this risk when the patients at risk of myocarditis would likely develop the condition anyway, that choice ultimately does not confer a benefit and weakens the population’s and the patient’s protection against COVID-19. For instance, dilated cardiomyopathy has a strong genetic basis. It’s not hard to imagine that a viral trigger can initiate the condition or make it apparent and if an individual already has the pathogenic genetic variants associated with this, withholding vaccination will likely to very little to modify their future risk of getting myocarditis or dilated cardiomyopathy but will mean they forgo protection against COVID-19 (which could be among the viral syndromes that initiate that destructive cascade).
It is worth discussing the history of vaccines and myocarditis. In general, vaccines are not associated with myocarditis with the exception of the smallpox vaccine. It is true that you can find case reports of myocarditis after many different vaccines, but as far as epidemiological evidence, only the smallpox vaccine has been shown to be a cause of myocarditis (and note that because of how many different things cause myocarditis, isolated case reports need to be considered with the possibility that they reflect coincidental events). Many vaccine-preventable diseases are causes of myocarditis and vaccination is a key means by which we can prevent myocarditis from those diseases. There has been some literature claiming that influenza vaccines are associated with myocarditis but in my review of the literature I in fact found the opposite to be true. For instance in a population of patients who were on immune checkpoint inhibitors, those who were vaccinated against influenza had both a lower risk of myocarditis and of the cases that did occur, the severity was milder (though this is correlative data and thus should not be presumed to be causal but the finding is consistent across two studies of the patient population; influenza vaccines have well documented cardiovascular benefits related to their ability to prevent influenza). The risk of myocarditis following the smallpox vaccine was found to be increased by about 200 times compared with baseline (though there’s a lot of uncertainty about that estimate but it is definitely significantly elevated) and asymptomatic increases in troponin after smallpox vaccination is as high as 28.7 per 1000 (and given that frequency I think it is worth being circumspect about the potential meaning of an elevated troponin in myocarditis from an mRNA vaccination against COVID-19). Some data is even more dramatic, suggesting that among those who were immunologically naive, the vaccine was associated with myopericarditis in 1 per 175 people- though fortunately the vast majority of cases were mild, self-resolving, and did not progress into DCM. Smallpox vaccine myocarditis typically occurs 6 to 12 days after the vaccination, and in biopsies it appears to be a lymphocytic-eosinophilic myocarditis, and this myocarditis was (very rarely) at times fatal to recipients of the smallpox vaccine, and it did sometimes progress into dilated cardiomyopathy. Because of the timing and the nature of the vaccine, this does not likely reflect what is happening with the mRNA vaccines; we know for instance that in viral myocarditis much of the damage that occurs is directly the result of both the virus infecting the heart and the immune response against it. Here there is no virus to speak of, no active replication of antigens beyond the short window of time preceding degradation of the mRNA. The smallpox vaccines are live attenuated, and potentially could infect the heart directly and provoke myocarditis in that manner (that would be consistent with the timing of the condition); we know that viral persistence is associated with more severe forms of myocarditis and progression to DCM. Furthermore, the quantities of spike protein found in the plasma are not plausibly high enough to cause myocarditis as seen here (and this isn’t observed with other types of vaccines containing spike protein thus far nor has it been documented as a pathologic effect from the spike protein in general), and pharmacokinetic and biodistribution data suggest that the vascular leak of the vaccine (mRNA at least) is minimal, which begs the question of what it is from the vaccine that could be provoking the response as these data suggest it’s not likely to be the direct effect of vaccine components. Certainly, the effect could be cytokine-mediated and a result of reactogenicity, but the mechanistic details are elusive. Some of the literature is referring to the vaccine-associated myocarditis as a hypersensitivity myocarditis, but some other authors do not believe the etiology is hypersensitivity-mediated because of a consistent absence of peripheral eosinophilia as would be typical for hypersensitivity myocarditis (though peripheral eosinophilia does not always occur with hypersensitivity myocarditis). Today, the smallpox vaccine is only given to members of the military because of bioterrorism concerns, as the pathogen is eradicated.
ACIP’s most recent recommendations regarding myocarditis and the mRNA vaccine. The last one regarding a reaction following the first dose has been met with some considerable opposition from clinicians but I am puzzled as to why this is. The recommendation is very soft and emphasizes shared decision-making. There are conditions in which the risk of COVID-19 may be so great that the potential benefits of that second dose exceed the potential risks. That isn’t going to apply to most people but the option is left open for the minority who do, and similarly the choice not to get the second dose is also left open with appropriate discussion.
The dilemma we are tasked with is how to maximize the benefit and minimize the harm from COVID-19 vaccination, particularly in adolescents (and ACIP has addressed this). Among the groups at risk, 12-17 year old males were observed to have the greatest risk of myocarditis, estimated at about 1 per 15,000 second doses of mRNA (in this case Pfizer/BioNTech because that’s the only one available for that age group) vaccine in the VAERS data. The obvious question to start with is how this risk compares to that from COVID-19 but this is not a simple question. Despite the rhetoric throughout the pandemic, COVID-19 can be serious in children, as I have discussed before here and here. COVID-19 is, to the best of our knowledge, a much less concerning disease in children than it is for adults but it still has a substantial public health burden, can cause profound morbidity, and our understanding of its risks in children is incomplete. To start with, we should consider whether or not the risks of the disease exceed the risks of the vaccination and so I’ll begin by considering MIS-C which is infamous for its cardiac involvement. MIS-C is an extremely severe illness: 43.2% of patients in this systematic review presented with shock, 39.3% required inotropic support, and 23.5% needed mechanical ventilation, and 2.2% needed ECMO. It has been estimated to occur in about 1 per 3000 SARS-CoV-2 infections. It is also estimated that among MIS-C patients (in addition to myriad other problems) myocarditis incidence may range from 75.3% to 41.4%, giving a range of about 1 per 7000 to 1 per 4000 SARS-CoV-2 infections that produce myocarditis among children. Certainly, some will look at this and point out that this value is smaller than the frequencies noted in Israel among their 16-24 year old males, which isn’t untrue, but because of how many different things can cause myocarditis and differences in exposures, daily activities (e.g. army training), I am not as comfortable generalizing the Israeli data to the US population. The risk is noted to be disproportionately high among Black and Hispanic children, likely reflecting a greater likelihood of becoming infected owing to structural racism, and the severity of the initial COVID-19 case is not predictive of whether or not a child develops MIS-C (indeed the initial cases are often asymptomatic and when MIS-C is found, a serology shows prior SARS-CoV-2 infection). However, already, this risk is higher than the risk from the group at highest risk from myocarditis associated with the mRNA vaccines as of the numbers currently available in the US.
COVID-19 also carries a risk of causing myocarditis acutely (and SARS-CoV-2 shows tropism for the heart and has been isolated from patients), but the frequency with which this occurs is harder to determine, especially in children in whom cases may be milder or asymptomatic (myocarditis can be asymptomatic too). However, among athletes the risk of myocarditis following acute COVID-19 was found to be as high as 2.3%, though this number needs to be interpreted with caution: some of the cases may reflect abnormalities due to the athletic heart’s own remodeling and because the patients were not followed longitudinally, other causes for their myocarditis cannot be excluded. Furthermore, there wasn’t a control group in this study that did not have COVID-19 to allow for reliable estimates of the risk increase in myocarditis compared with other causes. Another study using CMR on athletes who recovered from COVID-19 found 1.4% of them had evidence of myocarditis, but there were relatively few cases examined so there is significant uncertainty in that estimate, and it is subject to many of the same caveats that the previously mentioned study on athletes is. Additionally, both of these studies focus on an age group which is higher than the one we are presently interested in (12-17 years old), which may render generalizations about the risk of myocarditis from COVID-19 acutely inappropriate. However, based on available evidence, it is hard to argue that COVID-19 does not present a greater risk for myocarditis than do mRNA vaccines for COVID-19, and COVID-19 carries many additional risks that mRNA vaccines lack. As Dr. Sallie Permar (pediatrician-in-chief at Weill Cornell Medicine) states:
“If you think about all the risks that come with getting COVID itself, those are way more common” than the very low myocarditis rates we’re seeing with vaccines, Permar told me. “If you’re playing the numbers, every time you would choose to vaccinate your child to prevent disease.”
Dr. Permar is not alone in this opinion (and did proceed to vaccinate her 12-year-old son). In fact, a statement was issued cosigned by numerous leaders in public health and medicine supporting this exact point. If those aren’t enough for you, you may want to consider the opinion of Dr. Leslie T. Cooper Jr, who has authored about half of my references for this post and is possibly the world’s leading expert on myocarditis:
Of course, this is subject to a question which introduces a moral hazard: what is the likelihood of any given child in the US in this age group getting COVID-19? That question is perhaps even harder to answer because SARS-CoV-2’s attack rates in any given community are dynamic, and novel variants are constantly emerging, with potential for increased transmissibility over time as observed most prominently with the delta variant. This is why it frustrates me when people look at the low rates of hospitalization in children in the US currently as a reason not to vaccinate them. The low rates of hospitalization are certainly a good thing and I am very relieved to see them, but it takes time to build immunity and if we wait until they rise again, as they are expected to with the change in the season, then many children will be harmed by COVID-19, particularly if we want to relax mitigation measures in schools (which I think is worth doing provided that the children are vaccinated)- and it will have been completely preventable. The problem with this question more broadly, however, is it attempts to treat vaccination against an infectious disease as a purely medical problem when it is also a matter of public health (shall we spend a moment contemplating how individualistic thinking throughout this pandemic has harmed us all?). For instance, what if we applied this thinking to polio? The risk of a polio case in the US, or virtually anywhere else in the world at the time of writing this is very nearly zero (the exceptions being the few remaining endemic nations). One could easily make the argument that we could arrest polio vaccination because though IPV is a very safe vaccine, it is not without risk (e.g. anaphylaxis) and what’s the point, per this line of reasoning, if any given child in most of the world is unlikely to ever get polio? The issue is, arresting IPV vaccination before polio is eradicated would create optimal conditions for a resurgence of the disease after adequate loss of immunity e.g. from population turnover. It’s not an accident that in the pre-vaccine era for measles for instance, there were large outbreaks every 3 to 5 years: your immune patients died and you had susceptible patients born, and the virus circulated at low levels in the community until conditions were optimal for outbreak which occurred every few years. Looking at the rates of disease and infection now is misleading regarding future risk if we elect not to take steps to protect children from COVID-19.
Returning to the delta variant, there is a model which we can reference for our thought experiment on US complacency: the UK. Technical briefing documents from the UK show that schools are a consistent source of outbreaks from the delta variant and that school age children (predominantly older ones) show a high propensity for becoming infected. This is entirely predictable: if everyone else is immune to this virus, who is left as a susceptible host? The swathes of unvaccinated children (and they do transmit virus onward with similar efficiency to adults after you adjust for all confounders). Delta is poised to become dominant in the US as well, and some back of the envelope math from Professor Trevor Bedford estimates that it might cause as many as 36 million new infections therein, its effects even being seen now in Missouri within undervaccinated communities. A substantial portion of new infections will be in children as they may be too young to be vaccinated, or have simply had less opportunity to do so in terms of time. Professor Christina Pagel summarizes the trajectory of the pandemic in the UK in this thread, and it is undeniably concerning. Cases are rising precipitously in a highly vaccinated population, preferentially seeking out younger adults and children (because they aren’t vaccinated). Undeniably though, the vaccines are working as hospitalizations have been much slower to rise (the vaccination rates among older individuals in the UK are very high and these are the ones most likely to be hospitalized), and this should ease strain on the NHS. Israel also experienced a small surge from the delta variant that caused it to reinstate masking in public despite its very high rate of vaccination. It is worth noting that in view of the myocarditis, Israel initially balked when it came to vaccination of its 12- to 15-year-olds given very low cases counts. R0 for the variant has been estimated to be as high as 8, and if this is true, the minimal vaccine efficacy against transmission to bring R to 1 for this variant is 87.5%, under the assumption that everyone is to be vaccinated and generates a protective response (which in practice, is not going to be feasible because people may be immunocompromised or contraindicated from vaccination). Public Health England’s preprint has measured an effectiveness of 88% against symptomatic disease using 2 doses of the Pfizer vaccine- which means efficacy against transmission is likely lower. That really does not offer much wiggle room at all.
Still, if we can reduce the risk of myocarditis, even if the vast majority of cases are mild and appear to self-resolve, that is worth doing. After polio had been eliminated from the US, the oral polio vaccine was judged unnecessary as even though it did a superior job of blocking transmission compared with the inactivated vaccine, it very rarely could cause paralytic polio, and there was a suitable alternative with the inactivated polio vaccine that could not do this. The trouble here is that such considerations need to be grounded in data and there presently isn’t any sufficient to make confident judgments. For example, it has been noted that younger children frequently mount more robust immune responses and this is in fact why for those under 15, only 2 doses of HPV vaccine are needed instead of 3. Thus some have argued that it should be sufficient for now to give a single dose of mRNA vaccine as the risk of myocarditis is markedly lower from dose 1 based on available data. Now, this would certainly reduce the risk of myocarditis associated with the mRNA vaccines but the issue here is it means inferior protection against COVID-19. Some have countered this point by referencing effectiveness data from Public Health England showing that a single dose of Pfizer vaccine is 94% effective against the delta variant- but what is often left out of that soundbite is that the 95% confidence interval for this estimate is very wide (46-99), meaning there is great uncertainty about this estimate. Furthermore, from this same dataset, the effectiveness of a single dose of Pfizer vaccine against symptomatic disease is just 36%. It’s true that at the public health level (in the immediate term) preventing hospitalizations is most critical as it ensures that the healthcare system does not collapse, but given the panoply of post-acute consequences associated with COVID-19 (for instance those from the UK biobank study), I personally do not feel comfortable with a single dose approach without additional data. Furthermore, a 2-dose series for the HPV vaccine is still a prime-boost series, while a single dose of mRNA vaccine as a series has no boost. In vaccinology, it is generally only live attenuated vaccines which are highly effective even with just a single dose (and even then sometimes you need the second dose to achieve adequate immunity in the population because the pathogens in question are so contagious), thought to be related to the fact that they have limited replication within the body, which mRNA vaccines are not and do not. There are questions about whether or not a single dose of vaccine is adequate for ensuring memory responses that are required for durable protection. The early phases of the clinical trial process examined immunogenicity and tested doses and schedules to deduce which ones maximized immunogenicity and minimized reactogenicity- the choice of 2 doses with 30 mcg of mRNA is grounded in data. If this provides inadequate protection against COVID-19 (and to the best of my knowledge we don’t have data to substantiate the performance of a single dose of vaccine in these age groups or evidence of anamnestic responses with a single dose), then the calculus of risks and benefits gets more murky with this approach. I do think that there is a pertinent caveat here though and that has to do with a single dose for patients who have recovered. Multiple studies show that a boost effect is readily achieved with a single dose of mRNA vaccine that is superior to the immunity conferred from a complete series in a naive patient or from recovery from infection, and further that a second boost is not apparent with a second dose. I therefore think it is reasonable that in those who have documented prior infection that it is appropriate to use a single vaccine dose, especially given the risk of myocarditis. I will add though that I do not think that routine screening with serologies to confirm prior infection is wise as a basis for determining the number of doses because of issues with the positive predictive value of that endeavor (pre-test probability is a challenge in kids especially because their initial cases can be so mild) and operationalizing such a system would prove very difficult.
There is an arbitrary (sort of) component here though, and that would be the dosing interval. Classically, in vaccinology, giving prime-boost doses less than 3 weeks apart results in the first dose interfering with the immune response to the second and reduces vaccine efficacy- hence why Pfizer/BioNTech’s vaccine is given 3 weeks apart. A longer interval is actually associated with better antibody responses, but comes at the expense of a longer period of vulnerability given incomplete protection from a single dose. Certainly, a longer interval is easily justified when SARS-CoV-2 attack rates are low, but does it reduce the risk of vaccine-associated myocarditis? We don’t have any data either way. The pathophysiology of the vaccine-associated cases of myocarditis is not currently known. How can we be sure that the more robust immune response caused by a longer dosing interval does not in fact increase risk or enhance the severity of myocarditis cases? I can’t think of a reason we can be confident in this. Additionally, as more transmissible variants emerge, it may become even more important to vaccinate as quickly as possible, which further complicates the suggestion to extend dosing intervals if it is to become standard.
The most interesting solution I have seen proposed and the one I think is potentially most viable is that among those above age 18, one could do a heterologous series with a second dose of Johnson and Johnson/Janssen’s vaccine after an initial dose of mRNA vaccine. Mounting data are reassuring regarding the safety of heterologous series and there is potential for an immunologic advantage, so from the perspective of principles, this sounds promising. However, there are two issues here still: firstly that this approach cannot be applied to those under age 18 for now as EUA has not been granted for the Janssen vaccine in those under that age group, and from a regulatory perspective it sets a concerning precedent to extend the EUA to children when the product has not been evaluated in children yet. This is a fundamental issue here: there is no alternative vaccine available to the pediatric population other than the Pfizer/BioNTech vaccine. The other problem is of course, the lack of data to show that this reduces the risk of myocarditis. I think it’s likely as the Janssen vaccine has not been associated with this risk, but because the mechanism by which the myocarditis arises is not known, it’s hard to be confident about the matter (for instance, if the myocarditis is a reactogenicity-driven process, heterologous series may make things worse; if it’s related to priming from the mRNA vaccines that’s occurring anyway if you do that dose first), though I do think this approach is likely superior to the two aforementioned.
I should mention that I am not arguing that these hypotheses for how to reduce myocarditis risk should not be explored; in fact I think it’s absolutely critical that they are. But we should have a high standard for recommendations on the use of these vaccines and insofar as there are really obvious ways that each of these options may actually make things worse, I don’t think recommending any of them is appropriate without additional data.
In the interim, we should focus on what is currently known:
Myocarditis is a rare outcome, irrespective of age and sex.
In most cases, it rapidly resolves, though we will need continued follow up of patients to know more.
Immunological profiling of some patients shows an NK cell elevation which have a protective role in viral myocarditis by preventing fibrotic changes driven by eosinophils and autoreactive T cells that result in progression to DCM.
COVID-19 is much riskier even if you consider just the risks of myocarditis and not any of the other problems it can cause.
Work is actively underway to better understand this risk and how to mitigate it.
Given the available evidence, I personally believe that the ACIP was largely right in its recommendations.
I understand that given all this uncertainty some may argue that precautionary principles should predominate and vaccination of adolescents should be paused until we can get more clarity here, but precautionary principles have infamously led vaccination programs astray in the past (thimerosal comes to mind as an example- there was never any credible evidence of harm, but it was removed to ease anxieties, only serving to confirm for some people that it was dangerous in the first place and undermine trust in vaccination and also forcing the use of single-dose vials for routine immunizations). Pausing here means leaving kids vulnerable to COVID-19 and with the delta variant showing such a penchant for the unvaccinated as well as a heightened risk of hospitalization compared with alpha which itself was associated with a heightened risk of hospitalization, waiting for more information has serious potential for cause significant harm and it’s unclear whether it will be compensated for with apparent good.
I would love an alternative option that reduces the risk here but there currently isn’t one, and I am deeply troubled by the certainty with which some have been arguing for certain changes to how the vaccine is given without solid data to inform this.
Acknowledgments
I am deeply indebted to pediatric cardiologist Dr. Frank Han, MD for his extraordinary thoroughness in reviewing this post and editorial oversight.
References
1.Fuster V, Harrington RA, Narula J, Eapen ZJ. Hurst’s the heart, 14th edition: Two volume set. 14th ed. McGraw-Hill Education/Medical; 2017.
2.Zipes DP, Libby P, Bonow RO, Mann DL, Tomaselli GF. Braunwald’s heart disease: A textbook of cardiovascular medicine, 2-volume set. 11th ed. Philadelphia, PA: Elsevier - Health Sciences Division; 2018.
3.Myocarditis Foundation. Understanding Myocarditis – Myocarditis Foundation [Internet]. Myocarditisfoundation.org. 2010 [cited 2021 May 24];Available from: https://www.myocarditisfoundation.org/about-myocarditis/?gclid=Cj0KCQjwna2FBhDPARIsACAEc_X7rtwGiJHytBIGQzbrH9U9L1-aupz-Y7iYJxfnOsaS5gqJtvzvzrsaAjqMEALw_wcB
4.Fung G, Luo H, Qiu Y, Yang D, McManus B. Myocarditis. Circ Res 2016;118(3):496–514.
5.Kawakami R, Sakamoto A, Kawai K, et al. Pathological evidence for SARS-CoV-2 as a cause of myocarditis: JACC review topic of the week. J Am Coll Cardiol 2021;77(3):314–25.
6.Fish AE, Pride YB, Pinto DS. Lyme carditis. Infect Dis Clin North Am 2008;22(2):275–88, vi.
7.Olejniczak M, Schwartz M, Webber E, Shaffer A, Perry TE. Viral myocarditis—incidence, diagnosis and management. J Cardiothorac Vasc Anesth 2020;34(6):1591–601.
8.Awadalla M, Golden DLA, Mahmood SS, et al. Influenza vaccination and myocarditis among patients receiving immune checkpoint inhibitors. J Immunother Cancer 2019;7(1):53.
9.Morgan J, Roper MH, Sperling L, et al. Myocarditis, pericarditis, and dilated cardiomyopathy after smallpox vaccination among civilians in the United States, January-October 2003. Clin Infect Dis 2008;46 Suppl 3(s3):S242-50.
10.Tschöpe C, Ammirati E, Bozkurt B, et al. Myocarditis and inflammatory cardiomyopathy: current evidence and future directions. Nat Rev Cardiol 2021;18(3):169–93.
11.Cooper LT Jr. Myocarditis. N Engl J Med 2009;360(15):1526–38.
12.Pollack A, Kontorovich AR, Fuster V, Dec GW. Viral myocarditis--diagnosis, treatment options, and current controversies. Nat Rev Cardiol 2015;12(11):670–80.
13.COVID-19 VaST technical report may 17, 2021 [Internet]. Cdc.gov. 2021 [cited 2021 May 24];Available from: https://www.cdc.gov/vaccines/acip/work-groups-vast/technical-report-2021-05-17.html
14.Bajaj R, Sinclair HC, Patel K, et al. Delayed-onset myocarditis following COVID-19. Lancet Respir Med 2021;9(4):e32–4.
15.Arola A, Pikkarainen E, Sipilä JO, Pykäri J, Rautava P, Kytö V. Occurrence and features of childhood myocarditis: A nationwide study in Finland. J Am Heart Assoc [Internet] 2017;6(11). Available from: http://dx.doi.org/10.1161/JAHA.116.005306
16.Kyto V, Arola A, Sipila J, Pikkarainen E, Rautava P. P2580Seasonality of myocarditis: a population based study in Finland. Eur Heart J [Internet] 2017 [cited 2021 May 24];38(suppl_1). Available from: https://academic.oup.com/eurheartj/article/38/suppl_1/ehx502.P2580/4089304
17.Bailey AL, Dmytrenko O, Greenberg L, et al. SARS-CoV-2 infects human engineered heart tissues and models COVID-19 myocarditis. JACC Basic Transl Sci 2021;6(4):331–45.
18.COVID-19 as a possible cause of myocarditis and pericarditis - American college of cardiology [Internet]. Acc.org. [cited 2021 May 24];Available from: https://www.acc.org/latest-in-cardiology/articles/2021/02/05/19/37/covid-19-as-a-possible-cause-of-myocarditis-and-pericarditis
19.Israel said probing link between Pfizer shot and heart problem in men under 30 [Internet]. Timesofisrael.com. [cited 2021 May 24];Available from: https://www.timesofisrael.com/israel-said-probing-link-between-pfizer-shot-and-heart-problem-in-men-under-30/
20.Gatti M, Raschi E, Moretti U, Ardizzoni A, Poluzzi E, Diemberger I. Influenza vaccination and myo-pericarditis in patients receiving immune checkpoint inhibitors: Investigating the likelihood of interaction through the Vaccine Adverse Event Reporting System and VigiBase. Vaccines (Basel) 2021;9(1):19.
21.Meeting Presentation. Vaccines and related biological products [Internet]. Fda.gov. [cited 2021 Jun 12];Available from: https://www.fda.gov/media/150054/download
22.Holder J. Tracking Coronavirus vaccinations around the world [Internet]. NY Times. 2021 [cited 2021 Jun 12];Available from: https://www.nytimes.com/interactive/2021/world/covid-vaccinations-tracker.html
23.Roth GA, Mensah GA, Johnson CO, et al. Global Burden of cardiovascular diseases and risk factors, 1990-2019: Update from the GBD 2019 Study. J Am Coll Cardiol 2020;76(25):2982–3021.
24.Leone O, Veinot JP, Angelini A, et al. 2011 consensus statement on endomyocardial biopsy from the Association for European Cardiovascular Pathology and the Society for Cardiovascular Pathology. Cardiovasc Pathol 2012;21(4):245–74.
25.Wu M-H, Wu E-T, Wang C-C, et al. Contemporary postnatal incidence of acquiring acute myocarditis by age 15 years and the outcomes from a nationwide birth cohort. Pediatr Crit Care Med 2017;18(12):1153–8.
26.Bachur RG, Shaw KN. Fleisher & Ludwig’s textbook of pediatric emergency medicine. 8th ed. Baltimore, MD: Wolters Kluwer Health; 2020.
27.Cihakova D, editor. Myocarditis. InTech; 2011.
28.Di Florio DN, Sin J, Coronado MJ, Atwal PS, Fairweather D. Sex differences in inflammation, redox biology, mitochondria and autoimmunity. Redox Biol 2020;31(101482):101482.
29.About Human Parvovirus B19 [Internet]. Cdc.gov. 2021 [cited 2021 Jun 15];Available from: https://www.cdc.gov/parvovirusb19/about-parvovirus.html
30.Blanco-Domínguez R, Sánchez-Díaz R, de la Fuente H, et al. A novel circulating MicroRNA for the detection of acute myocarditis. N Engl J Med 2021;384(21):2014–27.
31.Caforio ALP, Tona F, Bottaro S, et al. Clinical implications of anti-heart autoantibodies in myocarditis and dilated cardiomyopathy. Autoimmunity 2008;41(1):35–45.
32.Yeung C, Baranchuk A. Diagnosis and treatment of Lyme carditis: JACC review topic of the week. J Am Coll Cardiol 2019;73(6):717–26.
33.Sharma NC, Efstratiou A, Mokrousov I, Mutreja A, Das B, Ramamurthy T. Diphtheria. Nat Rev Dis Primers 2019;5(1):81.
34.Heymans S, Eriksson U, Lehtonen J, Cooper LT Jr. The quest for new approaches in myocarditis and inflammatory cardiomyopathy. J Am Coll Cardiol 2016;68(21):2348–64.
35.Myers JM, Cooper LT, Kem DC, et al. Cardiac myosin-Th17 responses promote heart failure in human myocarditis. JCI Insight [Internet] 2016;1(9). Available from: http://dx.doi.org/10.1172/jci.insight.85851
36.Nindl V, Maier R, Ratering D, et al. Cooperation of Th1 and Th17 cells determines transition from autoimmune myocarditis to dilated cardiomyopathy: Cellular immune response. Eur J Immunol 2012;42(9):2311–21.
37.Ammirati E, Veronese G, Bottiroli M, et al. Update on acute myocarditis. Trends Cardiovasc Med [Internet] 2020;Available from: http://dx.doi.org/10.1016/j.tcm.2020.05.008
38.Rose NR. Critical cytokine pathways to cardiac inflammation. J Interferon Cytokine Res 2011;31(10):705–10. 39.Borst O, Schaub M, Walker B, et al. CXCL16 is a novel diagnostic marker and predictor of mortality in inflammatory cardiomyopathy and heart failure. Int J Cardiol 2014;176(3):896–903.
40.Kuntz J, Crane B, Weinmann S, Naleway AL, Vaccine Safety Datalink Investigator Team. Myocarditis and pericarditis are rare following live viral vaccinations in adults. Vaccine 2018;36(12):1524–7.
41.Ong S, Rose NR, Čiháková D. Natural killer cells in inflammatory heart disease. Clin Immunol 2017;175:26–33. 42.Rose NR. Viral myocarditis. Curr Opin Rheumatol 2016;28(4):383–9.
43.Matoba R, Shikata I, Iwai K, et al. An epidemiologic and histopathological study of sudden cardiac death in Osaka Medical Examiner’s Office. Jpn Circ J 1989;53(12):1581–8.
44.Bolognesi M, Bolognesi D. Acute coronary syndrome vs. myopericarditis - not always a straightforward diagnosis. Am J Case Rep 2013;14:221–5.
45.Ong S, Rose NR, Čiháková D. Natural killer cells in inflammatory heart disease. Clinical Immunology 2017;175:26–33.
46.Sun JC, Lanier LL. NK cell development, homeostasis and function: parallels with CD8+ T cells. Nat Rev Immunol 2011;11(10):645–57.
47.Klion AD, Ackerman SJ, Bochner BS. Contributions of eosinophils to human health and disease. Annu Rev Pathol 2020;15(1):179–209.
48.Schultheiss H-P, Fairweather D, Caforio ALP, et al. Dilated cardiomyopathy. Nat Rev Dis Primers 2019;5(1):32.
49.Barin JG, Baldeviano GC, Talor MV, et al. Fatal eosinophilic myocarditis develops in the absence of IFN-γ and IL-17A. J Immunol 2013;191(8):4038–47.
50.Griseri T, Arnold IC, Pearson C, et al. Granulocyte macrophage colony-stimulating factor-activated eosinophils promote interleukin-23 driven chronic colitis. Immunity 2015;43(1):187–99.
51.Sharma AN, Stultz JR, Bellamkonda N, Amsterdam EA. Fulminant myocarditis: Epidemiology, pathogenesis, diagnosis, and management. Am J Cardiol 2019;124(12):1954–60.
52.Ammirati E, Cipriani M, Moro C, et al. Clinical presentation and outcome in a contemporary cohort of patients with acute myocarditis: Multicenter Lombardy registry: Multicenter Lombardy registry. Circulation 2018;138(11):1088–99.
53.Song T, Jones DM, Homsi Y. Therapeutic effect of anti-IL-5 on eosinophilic myocarditis with large pericardial effusion. BMJ Case Rep [Internet] 2017;2017. Available from: http://dx.doi.org/10.1136/bcr-2016-218992
54.McGeachy MJ, Cua DJ, Gaffen SL. The IL-17 family of cytokines in health and disease. Immunity 2019;50(4):892–906.
55.Lavine KJ, Pinto AR, Epelman S, et al. The macrophage in cardiac homeostasis and disease: JACC macrophage in CVD series (part 4). J Am Coll Cardiol 2018;72(18):2213–30.
56.Peretto G, Sala S, Rizzo S, et al. Arrhythmias in myocarditis: State of the art. Heart Rhythm 2019;16(5):793–801.
57.Nordenswan H-K, Lehtonen J, Ekström K, et al. Manifestations and outcome of cardiac sarcoidosis and idiopathic giant cell myocarditis by 25-year nationwide cohorts. J Am Heart Assoc 2021;10(6):e019415.
58.CV Physiology [Internet]. Cvphysiology.com. [cited 2021 Jun 25];Available from: https://www.cvphysiology.com/Heart%20Disease/HD002
59.Vermij SH, Abriel H, van Veen TAB. Refining the molecular organization of the cardiac intercalated disc. Cardiovasc Res 2017;113(3):259–75.
60.Gourdie RG. The cardiac gap junction has discrete functions in electrotonic and ephaptic coupling: Gap junction function in cardiac conduction. Anat Rec (Hoboken) 2019;302(1):93–100.
61.Palaskas N, Lopez-Mattei J, Durand JB, Iliescu C, Deswal A. Immune checkpoint inhibitor myocarditis: Pathophysiological characteristics, diagnosis, and treatment. J Am Heart Assoc 2020;9(2):e013757.
62.Cooper LT Jr, ElAmm C. Giant cell myocarditis. Diagnosis and treatment: Diagnosis and treatment. Herz 2012;37(6):632–6.
63.Tan JL, Fong HK, Birati EY, Han Y. Cardiac sarcoidosis. Am J Cardiol 2019;123(3):513–22.
64.Pagán AJ, Ramakrishnan L. The formation and function of granulomas. Annu Rev Immunol 2018;36:639–65.
65.Kandolin R, Lehtonen J, Salmenkivi K, Räisänen-Sokolowski A, Lommi J, Kupari M. Diagnosis, treatment, and outcome of giant-cell myocarditis in the era of combined immunosuppression. Circ Heart Fail 2013;6(1):15–22.
66.Mankad P, Mitchell B, Birnie D, Kron J. Cardiac sarcoidosis. Curr Cardiol Rep 2019;21(12):152.
67.Wu M-H, Wu E-T, Wang C-C, et al. Contemporary postnatal incidence of acquiring acute myocarditis by age 15 years and the outcomes from a nationwide birth cohort. Pediatr Crit Care Med 2017;18(12):1153–8.
68.Bennett JE, Dolin R, Blaser MJ. Mandell, Douglas, and bennett’s principles and practice of infectious diseases: 2-Volume set. 9th ed. Philadelphia, PA: Elsevier - Health Sciences Division; 2019.
69.Kaji M, Kuno H, Turu T, Sato Y, Oizumi K. Elevated serum myosin light chain I in influenza patients. Intern Med 2001;40(7):594–7.
70.Pericarditis in Children [Internet]. Chop.edu. [cited 2021 Jun 30];Available from: https://www.chop.edu/conditions-diseases/pericarditis-children
71.Kanai-Yoshizawa S, Sugiyama Kato T, Mancini D, Marboe CC. Hypersensitivity myocarditis and outcome after heart transplantation. J Heart Lung Transplant 2013;32(5):553–9.
72.Ahmed T, Goyal A. Endomyocardial Biopsy. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2021.
73.Murphy JG, Wright RS, Bruce GK, et al. Eosinophilic-lymphocytic myocarditis after smallpox vaccination. Lancet 2003;362(9393):1378–80.
74.Buttà C, Zappia L, Laterra G, Roberto M. Diagnostic and prognostic role of electrocardiogram in acute myocarditis: A comprehensive review. Ann Noninvasive Electrocardiol [Internet] 2020;25(3). Available from: http://dx.doi.org/10.1111/anec.12726
75.Causes of non ACS related troponin elevations - American college of cardiology [Internet]. Acc.org. [cited 2021 Jun 30];Available from: https://www.acc.org/latest-in-cardiology/articles/2014/07/18/13/16/causes-of-non-acs-related-troponin-elevations
76.Assomull RG, Lyne JC, Keenan N, et al. The role of cardiovascular magnetic resonance in patients presenting with chest pain, raised troponin, and unobstructed coronary arteries. Eur Heart J 2007;28(10):1242–9.
77.Canter CE, Simpson KE. Diagnosis and treatment of myocarditis in children in the current era. Circulation 2014;129(1):115–28. 78.Basso C, Calabrese F, Angelini A, Carturan E, Thiene G. Classification and histological, immunohistochemical, and molecular diagnosis of inflammatory myocardial disease. Heart Fail Rev 2013;18(6):673–81.
79.Chimenti C, Frustaci A. Contribution and risks of left ventricular endomyocardial biopsy in patients with cardiomyopathies: a retrospective study over a 28-year period. Circulation 2013;128(14):1531–41.
80.Ferreira VM, Schulz-Menger J, Holmvang G, et al. Cardiovascular magnetic resonance in nonischemic myocardial inflammation: Expert recommendations. J Am Coll Cardiol 2018;72(24):3158–76.
81.[Sciences/Pharmacokinetics] Do nano-particles of the Pfizer COVID-19 vaccine cross the blood-brain barrier and infect your brain with mRNA (or will fritz your gonads)? [Internet]. Wordpress.com. 2021 [cited 2021 Jul 2];Available from: https://scientistabe.wordpress.com/2021/05/31/sciences-pharmacokinetics-do-nano-particles-of-the-pfizer-covid-19-vaccine-cross-the-blood-brain-barrier-and-infect-your-brain-with-mrna-or-will-fritz-your-gonads/
82.MacIntyre CR, Mahimbo A, Moa AM, Barnes M. Influenza vaccine as a coronary intervention for prevention of myocardial infarction. Heart 2016;102(24):1953–6.
83.COVID-19 VaST technical report may 17, 2021 [Internet]. Cdc.gov. 2021 [cited 2021 Jul 2];Available from: https://www.cdc.gov/vaccines/acip/work-groups-vast/report-2021-05-17.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fvaccines%2Facip%2Fwork-groups-vast%2Ftechnical-report-2021-05-17.html
84.HAN Archive - 00443 [Internet]. Cdc.gov. 2021 [cited 2021 Jul 2];Available from: https://emergency.cdc.gov/han/2021/han00443.asp
85.Mandavilli A. Heart problems after vaccination are very rare, federal researchers say [Internet]. NY Times. 2021 [cited 2021 Jul 2];Available from: https://www.nytimes.com/2021/06/23/health/coronavirus-vaccine-heart.html
86.Myocarditis - NORD (national organization for rare disorders) [Internet]. Rarediseases.org. 2015 [cited 2021 Jul 2];Available from: https://rarediseases.org/rare-diseases/myocarditis/
87.Parry H, Bruton R, Stephens C, et al. Extended interval BNT162b2 vaccination enhances peak antibody generation in older people [Internet]. bioRxiv. 2021;Available from: https://www.medrxiv.org/content/10.1101/2021.05.15.21257017v1.full.pdf
88.Plotkin SA, Orenstein W, Offit PA, Edwards KM. Plotkin’s Vaccines. 7th ed. Philadelphia, PA: Elsevier - Health Sciences Division; 2017.
89.Fairweather D, Cooper LT Jr, Blauwet LA. Sex and gender differences in myocarditis and dilated cardiomyopathy. Curr Probl Cardiol 2013;38(1):7–46.
90.Vogel G. Israel reports link between rare cases of heart inflammation and COVID-19 vaccination in young men. Science [Internet] 2021 [cited 2021 Jul 2];Available from: https://www.sciencemag.org/news/2021/06/israel-reports-link-between-rare-cases-heart-inflammation-and-covid-19-vaccination
91.Related Biological Products. COVID-19 Vaccine Safety Updates [Internet]. Fda.gov. [cited 2021 Jul 2];Available from: https://www.fda.gov/media/150054/download
92.Engler RJM, Nelson MR, Collins LC Jr, et al. A prospective study of the incidence of myocarditis/pericarditis and new onset cardiac symptoms following smallpox and influenza vaccination. PLoS One 2015;10(3):e0118283.
93.Yeung C, Baranchuk A. Diagnosis and treatment of Lyme carditis. J Am Coll Cardiol 2019;73(6):717–26.
94.Wu L, Diny NL, Ong S, et al. Pathogenic IL-23 signaling is required to initiate GM-CSF-driven autoimmune myocarditis in mice. Eur J Immunol 2016;46(3):582–92.
95.Xie Y, Chen R, Zhang X, et al. Blockade of interleukin-17A protects against coxsackievirus B3-induced myocarditis by increasing COX-2/PGE2 production in the heart. FEMS Immunol Med Microbiol 2012;64(3):343–51.
96.Amoah BP, Yang H, Zhang P, Su Z, Xu H. Immunopathogenesis of myocarditis: The interplay between cardiac fibroblast cells, dendritic cells, macrophages and CD4+ T cells. Scand J Immunol 2015;82(1):1–9.
97.Pandey S, Rajasurya V. Nonviral Myocarditis. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2020.
98.Kumar K, Guirgis M, Zieroth S, et al. Influenza myocarditis and myositis: case presentation and review of the literature. Can J Cardiol 2011;27(4):514–22.
99.Lin Y-H, Platt M, Gilley RP, et al. Influenza causes MLKL-driven cardiac proteome remodeling during convalescence. Circ Res 2021;128(5):570–84.
100.Pizzini A, Burkert F, Theurl I, Weiss G, Bellmann-Weiler R. Prognostic impact of high sensitive Troponin T in patients with influenza virus infection: A retrospective analysis. Heart Lung 2020;49(1):105–9.
101.Hang W, Chen C, Seubert JM, Wang DW. Fulminant myocarditis: a comprehensive review from etiology to treatments and outcomes. Signal Transduct Target Ther 2020;5(1):287.
102.Cihakova D. Interleukin-10 stiffens the heart. J Exp Med 2018;215(2):379–81.
103.Bracamonte-Baran W, Čiháková D. Cardiac autoimmunity: Myocarditis. Adv Exp Med Biol 2017;1003:187–221.
104.Ong S, Ligons DL, Barin JG, et al. Natural killer cells limit cardiac inflammation and fibrosis by halting eosinophil infiltration. Am J Pathol 2015;185(3):847–61.
105.Douaud G, Lee S, Alfaro-Almagro F, et al. Brain imaging before and after COVID-19 in UK Biobank. medRxiv [Internet] 2021;Available from: https://www.medrxiv.org/content/10.1101/2021.06.11.21258690v2.full.pdf
106.Beijk MA, Vlastra WV, Delewi R, et al. Myocardial infarction with non-obstructive coronary arteries: a focus on vasospastic angina. Neth Heart J 2019;27(5):237–45.
107.Durani Y, Egan M, Baffa J, Selbst SM, Nager AL. Pediatric myocarditis: presenting clinical characteristics. Am J Emerg Med 2009;27(8):942–7.
108.Martins-Marques T, Hausenloy DJ, Sluijter JPG, Leybaert L, Girao H. Intercellular communication in the heart: Therapeutic opportunities for cardiac ischemia. Trends Mol Med 2021;27(3):248–62.
109.Blondiaux E, Parisot P, Redheuil A, et al. Cardiac MRI in children with multisystem inflammatory syndrome associated with COVID-19. Radiology 2020;297(3):E283–8.
110.Julia Stowe, Nick Andrews, Charlotte Gower, Eileen Gallagher, Lara Utsi, Ruth Simmons, Simon Thelwall, Elise Tessier, Natalie Groves, Gavin Dabrera, Richard Myers, Colin Campbell, Gayatri Arithalingam, Matt Edmunds, Maria Zambon, Kevin Brown, Susan Hopkins, Meera Chand, Mary Ramsay, Jamie Lopez Bernal. Effectiveness of COVID-19 vaccines against hospital admission with the Delta (B.1.617.2) variant [Internet]. Khub.net. [cited 2021 Jul 2];Available from: https://khub.net/web/phe-national/public-library/-/document_library/v2WsRK3ZlEig/view_file/479607329?_com_liferay_document_library_web_portlet_DLPortlet_INSTANCE_v2WsRK3ZlEig_redirect=https%3A%2F%2Fkhub.net%3A443%2Fweb%2Fphe-national%2Fpublic-library%2F-%2Fdocument_library%2Fv2WsRK3ZlEig%2Fview%2F479607266
111.RSV State Trends [Internet]. Cdc.gov. 2021 [cited 2021 Jul 2];Available from: https://www.cdc.gov/surveillance/nrevss/rsv/state.html
112.Foerster SR, Canter CE, Cinar A, et al. Ventricular remodeling and survival are more favorable for myocarditis than for idiopathic dilated cardiomyopathy in childhood: an outcomes study from the Pediatric Cardiomyopathy Registry. Circ Heart Fail 2010;3(6):689–97.
113.Taliercio CP, Olney BA, Lie JT. Myocarditis related to drug hypersensitivity. Mayo Clin Proc 1985;60(7):463–8.
114.Marshall M, Ferguson ID, Lewis P, et al. Symptomatic acute myocarditis in seven adolescents following Pfizer-BioNTech COVID-19 vaccination. Pediatrics 2021;e2021052478.
115.Watkins K, Griffin G, Septaric K, Simon EL. Myocarditis after BNT162b2 vaccination in a healthy male. Am J Emerg Med [Internet] 2021;Available from: https://www.sciencedirect.com/science/article/pii/S0735675721005362
116.Dufort EM, Koumans EH, Chow EJ, et al. Multisystem inflammatory syndrome in children in New York State. N Engl J Med 2020;383(4):347–58.
117.Dhar MS, Marwal R, Vs R, et al. Genomic characterization and Epidemiology of an emerging SARS-CoV-2 variant in Delhi, India [Internet]. bioRxiv. 2021;Available from: https://www.medrxiv.org/content/10.1101/2021.06.02.21258076v1.full.pdf
118.Li X, Ostropolets A, Makadia R, et al. Characterising the background incidence rates of adverse events of special interest for covid-19 vaccines in eight countries: multinational network cohort study. BMJ 2021;n1435.
119.O’Leary ST, Maldonado YA. Myocarditis after SARS-CoV-2 vaccination: True, true, and…related? Pediatrics 2021;e2021052644.
120.Mansour J, Short RG, Bhalla S, et al. Acute myocarditis after a second dose of the mRNA COVID-19 vaccine: a report of two cases. Clin Imaging 2021;78:247–9.
121.Singh B, Kaur P, Cedeno L, et al. COVID-19 mRNA Vaccine and Myocarditis. Eur J Case Rep Intern Med [Internet] 2021;Available from: http://dx.doi.org/10.12890/2021_002681
122.McLean K, Johnson TJ. Myopericarditis in a previously healthy adolescent male following COVID-19 vaccination: A case report. Acad Emerg Med [Internet] 2021;(acem.14322). Available from: http://dx.doi.org/10.1111/acem.14322
123.Vidula MK, Ambrose M, Glassberg H, et al. Myocarditis and other cardiovascular complications of the mRNA-based COVID-19 vaccines. Cureus [Internet] 2021 [cited 2021 Jul 2];13(6). Available from: https://www.cureus.com/articles/61030-myocarditis-and-other-cardiovascular-complications-of-the-mrna-based-covid-19-vaccines
124.Habib MB, Hamamyh T, Elyas A, Altermanini M, Elhassan M. Acute myocarditis following administration of BNT162b2 vaccine. IDCases 2021;25(e01197):e01197.
125.Navar AM, McNally E, Yancy CW, O’Gara PT, Bonow RO. Temporal associations between immunization with the COVID-19 mRNA vaccines and myocarditis: The vaccine safety surveillance system is working: The vaccine safety surveillance system is working. JAMA Cardiol [Internet] 2021 [cited 2021 Jul 2];Available from: https://jamanetwork.com/journals/jamacardiology/article-abstract/2781599
126.ACIP COVID-19 Vaccine Recommendations [Internet]. Cdc.gov. 2021 [cited 2021 Jul 2];Available from: https://www.cdc.gov/vaccines/hcp/acip-recs/vacc-specific/covid-19.html
127.Shay DK, Shimabukuro TT, DeStefano F. Myocarditis occurring after immunization with mRNA-based COVID-19 vaccines. JAMA Cardiol [Internet] 2021 [cited 2021 Jul 2];Available from: https://jamanetwork.com/journals/jamacardiology/fullarticle/2781600
128.Montgomery J, Ryan M, Engler R, et al. Myocarditis following immunization with mRNA COVID-19 vaccines in members of the US military. JAMA Cardiol [Internet] 2021 [cited 2021 Jul 2];Available from: https://jamanetwork.com/journals/jamacardiology/article-abstract/2781601
129.Kim HW, Jenista ER, Wendell DC, et al. Patients with acute myocarditis following mRNA COVID-19 vaccination. JAMA Cardiol [Internet] 2021 [cited 2021 Jul 2];Available from: https://jamanetwork.com/journals/jamacardiology/article-abstract/2781602
130.Abu Mouch S, Roguin A, Hellou E, et al. Myocarditis following COVID-19 mRNA vaccination. Vaccine 2021;39(29):3790–3.
131.Albert E, Aurigemma G, Saucedo J, Gerson DS. Myocarditis following COVID-19 vaccination. Radiol Case Rep 2021;16(8):2142–5.
132.Bautista García J, Peña Ortega P, Bonilla Fernández JA, Cárdenes León A, Ramírez Burgos L, Caballero Dorta E. Acute myocarditis after administration of the BNT162b2 vaccine against COVID-19. Rev Esp Cardiol (Engl Ed) [Internet] 2021;Available from: http://www.revespcardiol.org/en/linksolver/ft/pii/S1885-5857(21)00133-X
133.Keinath K, Church T, Kurth B, Hulten E. Myocarditis secondary to smallpox vaccination. BMJ Case Rep [Internet] 2018;2018. Available from: https://casereports.bmj.com/lookup/pmidlookup?view=long&pmid=29572367
134.Rosner CM, Genovese L, Tehrani BN, et al. Myocarditis temporally associated with COVID-19 vaccination. Circulation [Internet] 2021;Available from: http://dx.doi.org/10.1161/CIRCULATIONAHA.121.055891
135.D’Angelo T, Cattafi A, Carerj ML, et al. Myocarditis after SARS-CoV-2 vaccination: A vaccine-induced reaction? Can J Cardiol [Internet] 2021;Available from: https://linkinghub.elsevier.com/retrieve/pii/S0828-282X(21)00286-5
136.Minocha PK, Better D, Singh RK, Hoque T. Recurrence of acute myocarditis temporally associated with receipt of the mRNA COVID-19 vaccine in an adolescent male. J Pediatr [Internet] 2021;Available from: https://linkinghub.elsevier.com/retrieve/pii/S0022-3476(21)00617-X
137.Muthukumar A, Narasimhan M, Li Q-Z, et al. In depth evaluation of a case of presumed myocarditis following the second dose of COVID-19 mRNA vaccine. Circulation [Internet] 2021;Available from: http://dx.doi.org/10.1161/CIRCULATIONAHA.121.056038
138.Larson KF, Ammirati E, Adler ED, et al. Myocarditis after BNT162b2 and mRNA-1273 vaccination. Circulation [Internet] 2021;Available from: http://dx.doi.org/10.1161/CIRCULATIONAHA.121.055913
139.Miller ER, Moro PL, Cano M, Shimabukuro TT. Deaths following vaccination: What does the evidence show? Vaccine 2015;33(29):3288–92.
140.Technical briefing. SARS-CoV-2 variants of concern and variants under investigation in England [Internet]. Gov.uk. [cited 2021 Jul 2];Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/997414/Variants_of_Concern_VOC_Technical_Briefing_16.pdf
141.Peretto G, Sala S, Caforio ALP. Acute myocardial injury, MINOCA, or myocarditis? Improving characterization of coronavirus-associated myocardial involvement. Eur Heart J 2020;41(22):2124–5.
142.Tschöpe C, Cooper LT, Torre-Amione G, Van Linthout S. Management of myocarditis-related cardiomyopathy in adults. Circ Res 2019;124(11):1568–83.
143.Herman DS, Lam L, Taylor MRG, et al. Truncations of titin causing dilated cardiomyopathy. N Engl J Med 2012;366(7):619–28.
144.Tabish AM, Azzimato V, Alexiadis A, Buyandelger B, Knöll R. Genetic epidemiology of titin-truncating variants in the etiology of dilated cardiomyopathy. Biophys Rev 2017;9(3):207–23.
145.LeWinter MM, Granzier HL. Cardiac titin and heart disease. J Cardiovasc Pharmacol 2014;63(3):207–12.
146.News Division. Statement following CDC ACIP meeting from nation’s leading doctors, nurses, pharmacists and public health leaders on benefits of vaccination [Internet]. Hhs.gov. 2021 [cited 2021 Jul 2];Available from: https://www.hhs.gov/about/news/2021/06/23/statement-following-cdc-acip-meeting-nations-leading-doctors-nurses-public-health-leaders-benefits-vaccination.html
147.Grens K. Most kids with MIS-C report few or no COVID-19 symptoms: Study [Internet]. The-scientist.com. 2021 [cited 2021 Jul 2];Available from: https://www.the-scientist.com/news-opinion/most-kids-with-mis-c-report-few-or-no-covid-19-symptoms-study-68646
148.CDC/IDSA COVID-19 Clinician Call: Myocarditis After COVID-19 mRNA Vaccine; Plus Vaccine Q&A [Internet]. Idsociety.org. [cited 2021 Jul 2];Available from: https://www.idsociety.org/multimedia/clinician-calls/cdcidsa-covid-19-clinician-call-myocarditis-after-covid-19-mrna-vaccine-plus-vaccine-qa/
149.Marcos JCA. Delta variant ignites new mask debate [Internet]. The Hill. 2021 [cited 2021 Jul 2];Available from: https://thehill.com/policy/healthcare/561039-delta-variant-ignites-new-mask-debate
150.Wu KJ. Doctors are puzzled by heart inflammation in the young and vaccinated. Atl Mon [Internet] 2021 [cited 2021 Jul 2];Available from: https://www.theatlantic.com/health/archive/2021/07/vaccination-myocarditis-kids/619339/
151.Maron BJ, Udelson JE, Bonow RO, et al. Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities: Task force 3: Hypertrophic cardiomyopathy, arrhythmogenic right ventricular cardiomyopathy and other cardiomyopathies, and myocarditis: A scientific statement from the American heart association and American college of cardiology. Circulation 2015;132(22):e273-80.
152.West R, Kobokovich A, Connell N, Gronvall GK. COVID-19 antibody tests: A valuable public health tool with limited relevance to individuals. Trends Microbiol 2021;29(3):214–23. 1
53.Frieman M, Harris AD, Herati RS, et al. SARS-CoV-2 vaccines for all but a single dose for COVID-19 survivors. EBioMedicine 2021;68(103401):103401. 154.Craver R, Huber S, Sandomirsky M, McKenna D, Schieffelin J, Finger L. Fatal eosinophilic myocarditis in a healthy 17-year-old male with severe acute respiratory syndrome Coronavirus 2 (SARS-CoV-2c). Fetal Pediatr Pathol 2020;39(3):263–8.
155.Martinez MW, Tucker AM, Bloom OJ, et al. Prevalence of inflammatory heart disease among professional athletes with prior COVID-19 infection who received systematic return-to-play cardiac screening. JAMA Cardiol [Internet] 2021 [cited 2021 Jul 2];Available from: https://jamanetwork.com/journals/jamacardiology/fullarticle/2777308
156.Chung MK, Zidar DA, Bristow MR, et al. COVID-19 and cardiovascular disease: From bench to bedside: From bench to bedside. Circ Res 2021;128(8):1214–36.
157.Castiello T, Georgiopoulos G, Finocchiaro G, et al. COVID-19 and myocarditis: a systematic review and overview of current challenges. Heart Fail Rev [Internet] 2021;Available from: http://dx.doi.org/10.1007/s10741-021-10087-9
158.Starekova J, Bluemke DA, Bradham WS, et al. Evaluation for myocarditis in competitive student athletes recovering from Coronavirus disease 2019 with cardiac magnetic resonance imaging. JAMA Cardiol [Internet] 2021 [cited 2021 Jul 2];Available from: https://jamanetwork.com/journals/jamacardiology/fullarticle/2775372
159.Matsubara D, Kauffman HL, Wang Y, et al. Echocardiographic findings in pediatric multisystem inflammatory syndrome associated with COVID-19 in the United States. J Am Coll Cardiol 2020;76(17):1947–61.
160.Daniels CJ, Rajpal S, Greenshields JT, et al. Prevalence of clinical and subclinical myocarditis in competitive athletes with recent SARS-CoV-2 infection: Results from the big Ten COVID-19 Cardiac Registry: Results from the big ten COVID-19 cardiac registry. JAMA Cardiol [Internet] 2021 [cited 2021 Jul 2];Available from: https://jamanetwork.com/journals/jamacardiology/fullarticle/2780548
161.McMurray JC, May JW, Cunningham MW, Jones OY. Multisystem inflammatory syndrome in children (MIS-C), a post-viral myocarditis and systemic vasculitis-A critical review of its pathogenesis and treatment. Front Pediatr 2020;8:626182.
162.Hoste L, Van Paemel R, Haerynck F. Multisystem inflammatory syndrome in children related to COVID-19: a systematic review. Eur J Pediatr 2021;180(7):2019–34.
163.Payne AB, Gilani Z, Godfred-Cato S, et al. Incidence of multisystem inflammatory syndrome in children among US persons infected with SARS-CoV-2. JAMA Netw Open 2021;4(6):e2116420.
164.Cooper LT, Baughman KL, Feldman AM, et al. The role of endomyocardial biopsy in the management of cardiovascular disease: a scientific statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology: A scientific statement from the American heart association, the American college of cardiology, and the European society of cardiology. Circulation 2007;116(19):2216–33.
165.The Children’s Hospital of Philadelphia. Myocarditis [Internet]. Chop.edu. [cited 2021 Jul 2];Available from: https://www.chop.edu/conditions-diseases/myocarditis
166.Blauwet LA, Cooper LT. Myocarditis. Prog Cardiovasc Dis 2010;52(4):274–88.
167.Alsaied T, Tremoulet AH, Burns JC, et al. Review of cardiac involvement in multisystem inflammatory syndrome in children. Circulation 2021;143(1):78–88.
168.Aslan I, Fischer M, Laser KT, Haas NA. Eosinophilic myocarditis in an adolescent: a case report and review of the literature. Cardiol Young 2013;23(2):277–83.
169.Małek ŁA, Kamińska H, Barczuk-Falęcka M, et al. Children with acute myocarditis often have persistent subclinical changes as revealed by cardiac magnetic resonance. J Magn Reson Imaging 2020;52(2):488–96.
170.Kytö V, Sipilä J, Rautava P. The effects of gender and age on occurrence of clinically suspected myocarditis in adulthood. Heart 2013;99(22):1681–4.
171.O’Donohoe TJ, Ketheesan N, Schrale RG. Anti-troponin antibodies following myocardial infarction. J Cardiol 2017;69(1):38–45.
172.Tercatin R. COVID: Was Israel wrong not to vaccinate children ages 12-15 right away? [Internet]. The Jerusalem Post. 2021 [cited 2021 Jul 3];Available from: https://www.jpost.com/israel-news/covid-did-israel-screw-up-not-vaccinating-children-ages-12-15-right-away-672203
173.Meites E, Kempe A, Markowitz LE. Use of a 2-dose schedule for human Papillomavirus vaccination - updated recommendations of the Advisory Committee on Immunization Practices. MMWR Morb Mortal Wkly Rep 2016;65(49):1405–8.
174.Caraballo C, Desai NR, Mulder H, et al. Clinical implications of the New York Heart Association classification. J Am Heart Assoc 2019;8(23):e014240.
175.Gallagher J. Covid: Is there a limit to how much worse variants can get? [Internet]. BBC. 2021 [cited 2021 Jul 3];Available from: https://www.bbc.com/news/health-57431420
176.Elamm C, Fairweather D, Cooper LT. Pathogenesis and diagnosis of myocarditis. Heart 2012;98(11):835–40.
177.Shaddy P, Shaddy C. Moss & Adams’ heart disease in infants, children, and adolescents: Including the fetus and young adult. 10th ed. Baltimore, MD: Wolters Kluwer Health; 2021.
178.Berg J, Lovrinovic M, Baltensperger N, et al. Non-steroidal anti-inflammatory drug use in acute myopericarditis: 12-month clinical follow-up. Open Heart 2019;6(1):e000990.
179.Leiner T, Bogaert J, Friedrich MG, et al. SCMR Position Paper (2020) on clinical indications for cardiovascular magnetic resonance. J Cardiovasc Magn Reson [Internet] 2020;22(1). Available from: http://dx.doi.org/10.1186/s12968-020-00682-4
180.Kühl U, Pauschinger M, Schwimmbeck PL, et al. Interferon-β treatment eliminates cardiotropic viruses and improves left ventricular function in patients with myocardial persistence of viral genomes and left ventricular dysfunction. Circulation 2003;107(22):2793–8.
181.Maisch B. Cardio-immunology of myocarditis: Focus on immune mechanisms and treatment options. Front Cardiovasc Med [Internet] 2019;6. Available from: http://dx.doi.org/10.3389/fcvm.2019.00048
182.Seidel F, Holtgrewe M, Al-Wakeel-Marquard N, et al. Pathogenic variants associated with dilated cardiomyopathy predict outcome in pediatric myocarditis. Circ Genom Precis Med [Internet] 2021;Available from: http://dx.doi.org/10.1161/circgen.120.003250
183.Grading N. New York Heart Association [Internet]. Org.au. [cited 2021 Jul 3];Available from: https://www.heartonline.org.au/media/DRL/New_York_Heart_Association_(NYHA)_classification.pdf
184.Symptom and activity level assessment (outpatient setting) - American college of cardiology [Internet]. Acc.org. [cited 2021 Jul 3];Available from: https://www.acc.org/tools-and-practice-support/clinical-toolkits/heart-failure-practice-solutions/symptom-and-activity-level-assessment-outpatient-setting
185.Yedlapati SH, Khan SU, Talluri S, et al. Effects of influenza vaccine on mortality and cardiovascular outcomes in patients with cardiovascular disease: A systematic review and meta‐analysis. J Am Heart Assoc [Internet] 2021;10(6). Available from: http://dx.doi.org/10.1161/jaha.120.019636
186.Caforio ALP, editor. Myocarditis: Pathogenesis, Diagnosis and Treatment. 1st ed. Cham, Switzerland: Springer Nature; 2020.
187.Greenberg RN, Kennedy JS. ACAM2000: a newly licensed cell culture-based live vaccinia smallpox vaccine. Expert Opin Investig Drugs 2008;17(4):555–64.
188.Huang X, Sun Y, Su G, Li Y, Shuai X. Intravenous immunoglobulin therapy for acute myocarditis in children and adults: A meta-analysis. Int Heart J 2019;60(2):359–65.
189.Matucci A, Maggi E, Vultaggio A. Mechanisms of action of ig preparations: Immunomodulatory and anti-inflammatory effects. Front Immunol [Internet] 2015;5. Available from: http://dx.doi.org/10.3389/fimmu.2014.00690
190.Zipes DP, Jalife J, Stevenson WG. Cardiac electrophysiology: From cell to bedside. 7th ed. Philadelphia, PA: Elsevier - Health Sciences Division; 2017.
191.Jacobs J, Burke A. Eosinophilic Myocarditis: Differential Diagnosis on Endomyocardial Biopsy [Internet]. Lww.com. 2021 [cited 2021 Jul 4];Available from: https://journals.lww.com/pathologycasereviews/Fulltext/2021/05000/Eosinophilic_Myocarditis__Differential_Diagnosis.8.aspx
192.Takotsubo cardiomyopathy - NORD (national organization for rare disorders) [Internet]. Rarediseases.org. 2020 [cited 2021 Jul 4];Available from: https://rarediseases.org/rare-diseases/takotsubo-cardiomyopathy/
193.Coronado MJ, Bruno KA, Blauwet LA, et al. Elevated Sera sST2 is associated with heart failure in men ≤50 years old with myocarditis. J Am Heart Assoc 2019;8(2):e008968.
194.Arrigo M, Jessup M, Mullens W, et al. Acute heart failure. Nat Rev Dis Primers 2020;6(1):16.
195.Cardiac adverse events following smallpox vaccination --- United States, 2003 [Internet]. Cdc.gov. 2003 [cited 2021 Jul 5];Available from: https://www.cdc.gov/mmwr/preview/mmwrhtml/mm5212a2.htm
196.Faust JS, Mayes KD, Gounder C. Covid Is a Greater Risk to Young People Than the Vaccines [Internet]. NY Times. 2021 [cited 2021 Jul 5];Available from: https://www.nytimes.com/2021/07/04/opinion/covid-vaccine-kids-risks.html
197.Hall JE, Hall ME. Guyton and hall textbook of medical physiology. 14th ed. Philadelphia, PA: Elsevier - Health Sciences Division; 2020.
198.Lodish H, Berk A, Kaiser CA, et al. Molecular Cell Biology. 8th ed. New York, NY: W.H. Freeman; 2016.
199.Bautista-Rodriguez C, Sanchez-de-Toledo J, Clark BC, et al. Multisystem inflammatory syndrome in children: An international survey. Pediatrics 2021;147(2):e2020024554.
200.GRADE: Pfizer-BioNTech COVID-19 vaccine age 12-15 years [Internet]. Cdc.gov. 2021 [cited 2021 Jul 5];Available from: https://www.cdc.gov/vaccines/acip/recs/grade/covid-19-pfizer-biontech-vaccine-12-15-years.html
201.Bearse M, Hung YP, Krauson AJ, et al. Factors associated with myocardial SARS-CoV-2 infection, myocarditis, and cardiac inflammation in patients with COVID-19. Mod Pathol 2021;34(7):1345–57.
202.Nirenberg E, Hoshino R. Let’s recognize childhood COVID as the crisis it is [Internet]. MedpageToday. 2021 [cited 2021 Jul 5];Available from: https://www.medpagetoday.com/opinion/second-opinions/93055
203.Crotty S. Hybrid immunity. Science 2021;372(6549):1392–3.
204.Covid-19 vaccination in children - The BMJ [Internet]. Bmj.com. 2021 [cited 2021 Jul 5];Available from: https://blogs.bmj.com/bmj/2021/06/23/covid-19-vaccination-in-children/?utm_campaign=shareaholic&utm_medium=twitter&utm_source=socialnetwork
205.Costanzo LS. Physiology. 6th ed. Philadelphia, PA: Elsevier - Health Sciences Division; 2017.
206. Brambatti M, Matassini MV, Adler ED, Klingel K, Camici PG, Ammirati E. Eosinophilic myocarditis: Characteristics, treatment, and outcomes. J Am Coll Cardiol 2017;70(19):2363–75.
207. Gargano JW, Wallace M, Hadler SC, et al. Use of mRNA COVID-19 vaccine after reports of myocarditis among vaccine recipients: Update from the Advisory Committee on Immunization Practices - United States, June 2021. MMWR Morb Mortal Wkly Rep 2021;70(27):977–82.
208. Painter MM, Mathew D, Goel RR, et al. Rapid induction of antigen-specific CD4+ T cells guides coordinated humoral and cellular immune responses to SARS-CoV-2 mRNA vaccination [Internet]. bioRxiv. 2021 [cited 2021 Jul 10];2021.04.21.440862. Available from: https://www.biorxiv.org/content/10.1101/2021.04.21.440862v1
209. Sette A, Crotty S. Adaptive immunity to SARS-CoV-2 and COVID-19. Cell 2021;184(4):861–80.